Sayer Ji
Jul 30, 2025

Please comment on and share this Substack post on X: https://x.com/sayerjigmi/status/1950581120212353351
There's an old medical school joke that goes something like this: "The delivery of good medical care is to do as much nothing as possible." Samuel Shem wrote these words in his satirical novel The House of God back in 1978, intending them as dark humor about physician burnout and the absurdities of medical training.
But what if this wasn't a joke at all? What if it was prophecy?
As I write this in 2025, the American healthcare system consumes $4.8 trillion annually¹—more than the entire GDP of Germany. We have more specialists, more drugs, more procedures, and more sophisticated imaging technology than ever before in human history. And yet, by nearly every meaningful metric, we're sicker than ever. Chronic disease affects 60% of Americans². Mental health disorders have reached epidemic proportions³. And most damning of all: medical errors and correctly prescribed medications have become the third leading cause of death⁴.
The math is staggering. Each year, over 440,000 Americans die from preventable medical errors⁵. Another 128,000 die from properly prescribed pharmaceuticals⁶. That's more than half a million casualties annually from a system designed to heal. To put this in perspective, we lost 58,220 American lives during the entire Vietnam War. Our medical system kills that many people every six weeks.
But here's where the story takes an extraordinary turn. Just as this bloated, dangerous system reaches peak dysfunction, a quiet revolution is emerging from the most unlikely source: peer-reviewed medical journals. Study after study is revealing something that would have been heretical just a generation ago. Sometimes—often, in fact—doing nothing is not just safer than medical intervention. It's more effective.
The Day Everything Changed (And Nobody Noticed)
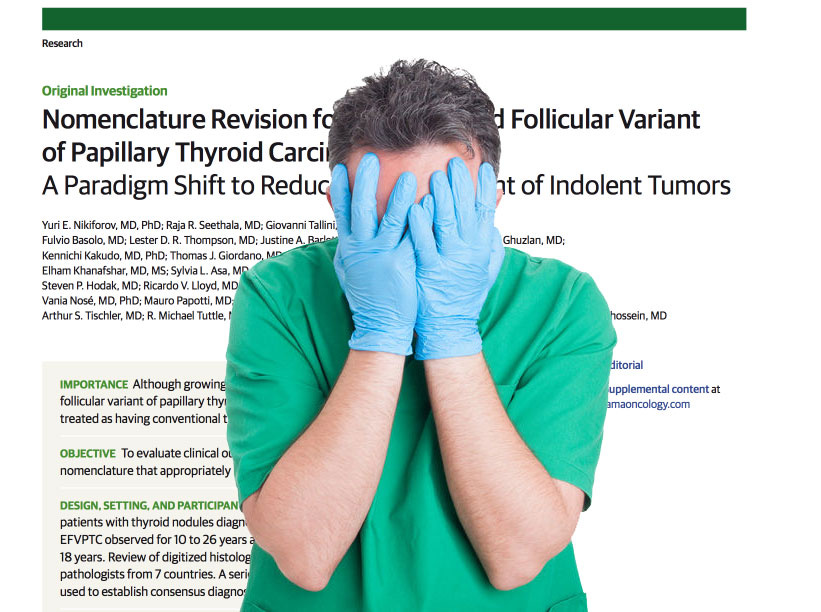
In 2013, something remarkable happened that should have made front-page news but instead was buried in the medical literature. A National Cancer Institute expert panel dropped what can only be described as an atomic bomb on the cancer industry. They concluded that millions of "cancers" we'd been aggressively treating—including ductal carcinoma in situ (DCIS) and high-grade prostatic intraepithelial neoplasia (PIN)—weren't actually cancers at all⁷.
Let that sink in for a moment. These conditions, which had been diagnosed as "breast cancer" and "prostate cancer" in millions of people, were reclassified as "benign or indolent lesions of epithelial origin." In plain English: harmless cellular changes that would never have caused symptoms or death if left alone.
The implications are staggering. A 2012 New England Journal of Medicine study estimated that 1.3 million American women had been wrongly treated for breast cancer over the previous three decades⁸. These women underwent surgeries, radiation, chemotherapy—with all their attendant suffering, disfigurement, and risk—for conditions that weren't actually threatening their lives.
You might expect such a revelation to transform medical practice overnight. You'd be wrong. More than a decade later, the same overdiagnosis and overtreatment continues largely unabated. Why? The answer reveals something profound about how our medical system operates—and why "doing nothing" has become, paradoxically, a radical act.
The $156 Billion Overtreatment Complex
Follow the money, as they say. The cancer screening and treatment industry generates roughly $156 billion annually in the United States alone⁹. Every mammogram that leads to a biopsy, every biopsy that leads to a lumpectomy, every lumpectomy that leads to radiation—each step in this cascade generates revenue. The average cost of breast cancer treatment can exceed $100,000¹⁰. Multiply that by hundreds of thousands of overdiagnosed cases, and you begin to understand why there's little institutional incentive to embrace watchful waiting.
But the costs aren't merely financial. There's a human price that can't be captured in spreadsheets. When a doctor tells you "You have cancer," something fundamental shifts in your psyche. Studies show that cancer patients have a significantly increased risk of suicide in the first year after diagnosis¹¹. Heart attack rates spike¹². Even when the "cancer" is successfully treated, the psychological wounds often never fully heal.
This is what researchers call the nocebo effect—placebo's evil twin. Where placebo harnesses belief to heal, nocebo weaponizes fear to harm. And modern medicine, with its culture of defensive practice and catastrophic thinking, has become a nocebo delivery system of unprecedented scale.
The Quantum Biology Revolution: Why Your Body Knows Better
To understand why "doing nothing" can be so powerful, we need to venture into the emerging field of quantum biology. Your body isn't just a collection of organs and tissues—it's a symphony of 50 trillion cells engaged in a constant dance of communication and self-regulation that operates on principles we're only beginning to understand.
Recent research has revealed that biological systems utilize quantum coherence—the same phenomenon that makes quantum computers possible—to perform feats that classical chemistry can't explain¹³. Photosynthesis, bird navigation, and possibly even consciousness itself depend on quantum effects. When we introduce pharmaceutical chemicals or surgical interventions into this exquisitely tuned system, we're not just affecting the target organ. We're disrupting a web of quantum relationships that took 3.8 billion years to evolve.
Consider your microbiome—the 100 trillion microorganisms that outnumber your human cells 10 to 1¹⁴. These aren't passive hitchhikers; they're active participants in your immune function, neurotransmitter production, and even gene expression. Every antibiotic, every medication, every medical procedure disrupts this ecosystem in ways we're only beginning to map. Sometimes the disruption is necessary. Often, it's not.
This is why the principle of "first, do no harm"—medicine's prime directive—has become more relevant than ever. In an age where we can do so much, the question isn't whether we can intervene, but whether we should.

The Mountain of Evidence: When Nothing Beats Everything
The evidence supporting non-intervention isn't anecdotal or fringe. It comes from the heart of the medical establishment itself: peer-reviewed, randomized controlled trials published in prestigious journals. Here's what decades of research reveals:
Spontaneous Healing: The Body's Hidden Superpower
Herniated Discs and Back Pain
The evidence here is particularly striking. A comprehensive meta-analysis published in Pain Physician found that the "incidence of spontaneous resorption of lumbar disc herniation is high"¹⁵. The study analyzed multiple trials and concluded that many herniated discs simply disappear on their own without any intervention.
Another study in Clinical Rehabilitation confirmed that "spontaneous regression of lumbar herniated discs is not uncommon"¹⁶. Researchers followed patients with MRI-confirmed disc herniations and found that the larger and more severe the herniation, the more likely it was to resolve spontaneously—completely contrary to conventional medical thinking.
Multiple case reports document complete resolution of cervical disc herniations verified by MRI¹⁷. One fascinating study showed that disc material that had actually separated from the main disc (sequestration) was most likely to be reabsorbed by the body¹⁸. The implications are profound: millions of back surgeries may be unnecessary.
Gallstone Disease
A meta-analysis in the Journal of Gastroenterology and Hepatology concluded that "expectant management (i.e. doing nothing) of gallstone disease is a valid therapeutic approach in the majority of patients"¹⁹. The researchers found that most people with gallstones never develop symptoms requiring intervention, and prophylactic surgery carries more risk than watchful waiting.
Childhood Ear Infections
Perhaps one of the most important studies for parents comes from Pediatrics, which found that "watchful waiting may be an acceptable alternative to immediate drug treatment for some children with nonsevere acute otitis media"²⁰. Children who were carefully monitored but not given antibiotics had the same recovery rates as those who received immediate antibiotic treatment—but they maintained their microbiome integrity and didn't contribute to antibiotic resistance.
Prostate Cancer
Long-term follow-up studies have revolutionized our understanding of prostate cancer. Research published in JAMAshowed that the majority of men diagnosed with low-grade prostate cancer will die with it, not from it²¹. Active surveillance—regular monitoring without treatment—preserves quality of life while maintaining equivalent survival rates to aggressive intervention.
Inguinal Hernias
A landmark study in JAMA compared watchful waiting to surgical repair for minimally symptomatic inguinal hernias. The results? No significant difference in outcomes, but the surgery group experienced complications that the watchful waiting group avoided²².
Even Liver Cancer
Remarkably, researchers have documented 61 cases of spontaneous regression of hepatocellular carcinoma between 1982 and 2006²³. While rare, these cases prove that even aggressive cancers can sometimes resolve without intervention—a phenomenon that challenges our fundamental understanding of cancer biology.

The Surgical Assault on Children's Immune Systems
While we're discovering that herniated discs, gallstones, and even some cancers resolve spontaneously, medicine continues its aggressive assault on healthy tissue—particularly in children. Consider the epidemic of tonsillectomies and adenoidectomies. For decades, these were among the most common surgeries performed on children, often for minor complaints like snoring or recurrent sore throats. A massive Danish study following 1.2 million children for up to 30 years has revealed the devastating long-term consequences of this "routine" surgery. Children who had their tonsils or adenoids removed showed significantly increased risks for 28 different diseases, including a 280% increased risk for upper respiratory diseases, doubled risk for COPD and asthma, and elevated risks for infectious, allergic, and psychiatric conditions⁵⁰. The tonsils and adenoids aren't vestigial organs to be casually discarded—they're critical components of the immune system, particularly during the developmental years. They serve as the body's first line of defense, training the immune system to recognize threats. Remove them, and you permanently alter a child's disease resistance for life. Yet despite this evidence, approximately 500,000 tonsillectomies are still performed annually in the United States alone, generating over $1.5 billion in revenue. Most could be avoided through watchful waiting, as the majority of children naturally outgrow tonsil and adenoid problems as their airways mature.

Natural Therapies That Outperform Pharmaceuticals
Light Therapy vs. Benzoyl Peroxide for Acne
A British Journal of Dermatology study found that blue and red light therapy cleared acne as effectively as 5% benzoyl peroxide—the gold standard topical treatment—but without the skin irritation, dryness, and bacterial resistance that comes with chemical intervention²⁴. The treatment is elegantly simple: specific wavelengths of light that kill acne bacteria and reduce inflammation.
Dietary Changes vs. Beta-Blockers for Hypertension
When researchers compared a high-fiber, low-sodium diet to the beta-blocker metoprolol in diabetic patients with high blood pressure, the results were striking. Not only did dietary changes match the drug's blood pressure reduction, but they also improved metabolic markers that the drug actually worsened²⁵. The patients eating real food got healthier overall; those taking the drug simply had lower blood pressure readings while their underlying health deteriorated.
Acupuncture vs. Conventional Treatment
Multiple studies have shown acupuncture matching or exceeding pharmaceutical interventions. For sudden deafness, acupuncture with moxibustion proved superior to standard drug therapy²⁶. For migraine prevention, acupuncture matched flunarizine (a calcium channel blocker) in effectiveness but with zero side effects²⁷. These aren't placebo effects—functional MRI studies show acupuncture creating measurable changes in brain activity²⁸.
Elemental Diets vs. Steroids for Crohn's Disease
When children with Crohn's disease were randomized to either an elemental diet (pre-digested nutrients that give the gut a rest) or high-dose steroids, both groups achieved similar remission rates. But the children on the elemental diet continued growing normally, while those on steroids suffered growth suppression—a devastating side effect in developing bodies²⁹. Three separate studies in adults found similar results³⁰.
Aromatherapy vs. Pain Medication
South Korean researchers studying menstrual pain in high school girls found that abdominal massage with lavender, clary sage, and marjoram oils reduced pain more effectively than acetaminophen³¹. The girls receiving aromatherapy also reported improved mood and decreased anxiety—benefits you won't find on a Tylenol label.
Hypnosis vs. Valium for Medical Procedures
French researchers studying women undergoing embryo transfer for IVF found that hypnosis matched diazepam (Valium) for reducing anxiety and improving pregnancy rates³². The difference? The hypnosis group avoided the risks of benzodiazepine dependence, cognitive impairment, and potential effects on the developing embryo.
Yogic Breathing vs. Antidepressants
In a remarkable study from India's National Institute of Mental Health, Sudarshan Kriya Yoga—a rhythmic breathing technique—was compared to both electroconvulsive therapy and imipramine (a tricyclic antidepressant) for major depression. The breathing technique matched the antidepressant in effectiveness and came close to ECT—psychiatry's "gold standard" for severe depression³³. No side effects. No risk of tardive dyskinesia or serotonin syndrome. Just breath.
Forest Bathing vs. Anxiolytics
Japanese researchers have extensively studied shinrin-yoku (forest bathing) and found it produces measurable improvements in immune function, stress hormones, and cardiovascular health³⁴. Natural killer cell activity increases by 50%. Cortisol drops significantly. Blood pressure normalizes. All from simply spending time among trees—no prescription required.

The Physics of Healing: Understanding Your Body's Operating System
To truly appreciate why "doing nothing" can be so powerful, we need to understand something fundamental about how healing actually works. Your body isn't a machine that needs fixing—it's a self-organizing system that's constantly working to maintain balance. Every second, without any conscious effort on your part:
Your bone marrow produces 2.5 million red blood cells
Your immune system identifies and destroys cancer cells before they can establish tumors
Your liver performs over 500 different functions
Your gut manufactures neurotransmitters that influence your mood
Your cells repair DNA damage from radiation and toxins
Your microbiome educates your immune system and produces vitamins
This isn't random biological activity. It's orchestrated intelligence that operates on multiple levels simultaneously—from the quantum interactions within proteins to the electromagnetic fields generated by your heart and brain. When you introduce pharmaceutical drugs into this system, you're not just affecting one pathway or organ. You're disrupting a network of relationships that we barely understand.
Consider what happens when you take a common proton pump inhibitor for acid reflux. Yes, it reduces stomach acid. But stomach acid exists for reasons beyond causing heartburn. It's essential for absorbing B12, magnesium, calcium, and iron. It's your first line of defense against foodborne pathogens. It triggers the cascade of digestive enzymes that break down proteins. Suppress it long-term, and you risk osteoporosis³⁵, dementia³⁶, kidney disease³⁷, and potentially even stomach cancer³⁸—the very condition these drugs were supposed to prevent.
This is the dirty secret of pharmaceutical intervention: every drug is a trade-off. You're accepting known and unknown risks in exchange for suppressing a symptom. Sometimes that trade-off is worthwhile. A diabetic in ketoacidosis needs insulin. A patient with acute appendicitis needs surgery. But for the vast majority of conditions that send people to doctors—chronic pain, digestive issues, mild hypertension, anxiety, insomnia—the trade-off often favors letting the body heal itself.

Your Body's Pharmacy: More Sophisticated Than Any Drug Company
Perhaps the most profound argument for doing nothing is that your body already contains the most sophisticated pharmacy imaginable. Consider:
Your brain produces its own opioids (endorphins) more powerful than morphine³⁹
Your gut manufactures 90% of your body's serotonin⁴⁰
Your skin synthesizes vitamin D from sunlight⁴¹
Your muscles release myokines during exercise that reduce inflammation throughout your body⁴²
Your vagus nerve, when activated through breathing or cold exposure, triggers a cascade of healing responses⁴³
Every pharmaceutical drug is essentially a crude attempt to mimic or block something your body does naturally. Statins interfere with cholesterol production. SSRIs block serotonin reuptake. Benzodiazepines enhance GABA. But your body's versions come with built-in feedback loops, safety mechanisms, and synergistic effects that no drug can replicate.
This internal pharmacy isn't theoretical. It's what allows placebo effects to work. When researchers give people sugar pills for pain, depression, or even Parkinson's disease, 30-70% show real improvement⁴⁴—not because they're gullible, but because the ritual of treatment activates their internal healing systems. The belief becomes biology.
The Revolutionary Practice of Intelligent Non-Intervention
So how do we actually "do nothing" in a culture obsessed with doing everything? It starts with changing our relationship to symptoms. In our pharmaceutical age, we've been trained to see every discomfort as a problem requiring intervention. Headache? Pop an ibuprofen. Can't sleep? Take an Ambien. Anxious? Here's a Xanax.
But symptoms aren't enemies—they're communications; messages of healing from deep within the native intelligence of your body and soul. Fatigue is your body asking for rest. Fever is your immune system creating an inhospitable environment for opportunistic ‘pathogens’ (or, if you dispute or disagree with classical germ theory, as I do, view my presentation on the topic at the link immediately below)
Genes, Germs, and the Myth of the Invisible Enemy: Toward a New Model of Health

"For over a century, the narratives of germ theory and genetic determinism have shaped the dominant view of health, casting invisible enemies—germs and faulty genes—as the primary causes of disease. This model, while persuasive, has fostered a culture of fear, disempowerment, and dependency, divorcing individuals from the deeper realities of health and …
Pain is a request to pay attention and perhaps change behavior. When we reflexively suppress these signals, we're essentially putting duct tape over the check engine light.
The 48-Hour Pause Protocol
Unless you're facing a true emergency, give yourself at least 48 hours before accepting any diagnosis or treatment plan. Use this time to:
Research the condition thoroughly, especially looking for "overdiagnosis + [condition name]"
Get second and third opinions, preferably from practitioners with different philosophies
Ask specific questions: What happens if we don't treat this? What's the natural history? How many people improve without intervention?
Request all your medical records and read them yourself
Look for watchful waiting protocols that might apply to your situation
The Cascade Prevention Strategy
Medical interventions rarely exist in isolation. One test leads to another. A borderline result triggers a biopsy. An incidental finding on a scan launches an investigation. At each step, ask:
What exactly are we looking for?
What will we do if we find it?
What happens if we don't look at all?
What are the false positive rates?
How many people are harmed by the investigation itself?
The Evidence Demand
When a doctor recommends intervention, ask for the research. Not their opinion or standard practice—actual studies showing that the intervention improves meaningful outcomes. You'll be surprised how often the evidence is weak, conflicting, or non-existent. Many common procedures continue based on tradition rather than proof of benefit. Always use independent resources like GreenMedInfo.com to do your own research and obtain information not freely available on Pharma funded websites and resources.
The Timeline Trust
Your body doesn't operate on medical scheduling. Healing happens in its own time. The arbitrary follow-up appointments and treatment timelines often have more to do with billing cycles than biology. If you're improving without intervention, keep doing nothing. Many conditions that seem urgent in the doctor's office resolve naturally given time.
The Active Waiting Practice
Doing nothing medically doesn't mean doing nothing at all. It means creating conditions for healing:
Sleep 7-9 hours in complete darkness
Eat real, unprocessed food that your great-grandmother would recognize
Move your body daily in ways that feel good
Manage stress through breathing, meditation, or time in nature
Connect with others who support your healing journey
Trust your body's timeline rather than arbitrary medical schedules
These aren't "alternative medicine"—they're the foundational medicine your body evolved to expect.
The Economics of Empowerment
When you choose watchful waiting over intervention, you're not just protecting your health—you're voting with your dollars against a predatory system. Consider the typical cascade of costs:
Suspicious mammogram: $200
Biopsy: $3,000
Lumpectomy: $15,000
Radiation: $25,000
Hormone therapy: $30,000 over five years
Total: $73,200
For a condition that, in many cases, would never have caused symptoms⁴⁵.
Multiply this by millions of overdiagnosed cases across dozens of conditions, and you begin to see why American healthcare costs twice as much as other developed nations while delivering worse outcomes⁴⁶. We're not paying for health—we're funding an intervention industry that profits from fear.
The Future of Doing Nothing
Imagine a healthcare system built on first principles. Where doing nothing is the default and intervention requires overwhelming evidence of benefit. Where practitioners are rewarded for keeping people healthy rather than treating disease. Where the nocebo effect is recognized and minimized rather than weaponized for profit.
This isn't utopian fantasy. It's already emerging in pockets around the world. Costa Rica's Blue Zones achieve better health outcomes at a fraction of US costs by focusing on lifestyle and community⁴⁷. Japan's forest therapy centers prescribe nature immersion covered by health insurance⁴⁸. Germany's month-long spa treatments address root causes rather than symptoms⁴⁹.
These models work because they align with biological reality: health is our default state when we provide proper conditions. Disease is usually the result of deficiency (nutrients, movement, connection) or excess (stress, toxins, medical intervention). Address these fundamentals and the body often heals itself.

The Choice That Changes Everything
We stand at perhaps the most important crossroads in medical history. Down one path lies more of the same: escalating intervention, rising costs, iatrogenic harm disguised as healthcare. Down the other lies something radically different: a return to trusting the 3.8-billion-year wisdom encoded in our cells.
This isn't about rejecting all medical care. Emergency medicine saves lives. Certain interventions are necessary and beneficial. But we must reclaim the discernment to know when to act and when to wait, when to intervene and when to trust, when to fear and when to have faith in our body's profound capacity for self-repair.
The revolution doesn't require protests or policy changes. It happens every time someone chooses watchful waiting over worried intervention. Every time someone addresses root causes rather than suppressing symptoms. Every time someone discovers that their body, given the right conditions, knows exactly how to heal.
The prescription has been written. It requires no pharmacy, no insurance approval, no medical authority. It's the radical act of doing nothing—intelligently, courageously, trusting that millions of years of evolution have equipped you with healing capabilities that make our most advanced pharmaceuticals look like stone tools.
Your body is waiting. Not for another drug or diagnosis or intervention, but for you to stop interfering with its ancient wisdom. To step back. To trust. To discover that sometimes the most powerful medicine is no medicine at all.
Please comment on and share this Substack post on X: https://x.com/sayerjigmi/status/1950581120212353351

HOW TO TAKE BACK FULL CONTROL OF YOUR HEALTH DESTINY
If you are interested in learning more about how to take full control of your health, my international bestselling book, now available in six languages, offers a comprehensive exploration of how we can activate our body's self-healing mechanisms through the New Biology. Get your copy here, or get a free chapter here.
The REGENERATE YOURSELF Masterclass
Join over 400,000 enrollees who have discovered practical ways to implement these groundbreaking concepts in their daily lives. This comprehensive online program translates cutting-edge science into actionable strategies for optimizing your health through the principles of the New Biology.
Enroll entirely free at: regeneratemasterclass.com Or, get the entire course including advanced modules here now.
Both resources provide practical tools and deeper scientific context for understanding how melanin, light, water, and other elements of the New Biology can be harnessed to unlock your body's extraordinary capacity for self-renewal and vitality.
Endnotes
Centers for Medicare & Medicaid Services, "National Health Expenditure Data," 2024, https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData.
Christine Buttorff, Teague Ruder, and Melissa Bauman, "Multiple Chronic Conditions in the United States," RAND Corporation, 2017, https://www.rand.org/pubs/tools/TL221.html.
National Institute of Mental Health, "Mental Health Statistics," 2023, https://www.nimh.nih.gov/health/statistics.
Martin A. Makary and Michael Daniel, "Medical error—the third leading cause of death in the US," BMJ 353 (2016): i2139, https://www.bmj.com/content/353/bmj.i2139.
John T. James, "A new, evidence-based estimate of patient harms associated with hospital care," Journal of Patient Safety 9, no. 3 (2013): 122-128, https://pubmed.ncbi.nlm.nih.gov/23860193/.
Donald W. Light, Joel Lexchin, and Jonathan J. Darrow, "Institutional corruption of pharmaceuticals and the myth of safe and effective drugs," Journal of Law, Medicine & Ethics 41, no. 3 (2013): 590-600, https://pubmed.ncbi.nlm.nih.gov/24088149/.
Laura J. Esserman et al., "Addressing overdiagnosis and overtreatment in cancer: a prescription for change," The Lancet Oncology 15, no. 6 (2014): e234-e242, https://pubmed.ncbi.nlm.nih.gov/24807866/.
Archie Bleyer and H. Gilbert Welch, "Effect of three decades of screening mammography on breast-cancer incidence," New England Journal of Medicine 367, no. 21 (2012): 1998-2005, https://www.nejm.org/doi/full/10.1056/nejmoa1206809.
Joann G. Elmore and Ruth Etzioni, "Effect of screening mammography on cancer incidence and mortality," JAMA Internal Medicine 175, no. 9 (2015): 1490-1491, https://pubmed.ncbi.nlm.nih.gov/26098711/.
American Cancer Society, "The Costs of Cancer," 2020 Edition, https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-treatment-and-survivorship-facts-and-figures/cancer-treatment-and-survivorship-facts-and-figures-2019-2021.pdf.
Fang Fang et al., "Suicide and cardiovascular death after a cancer diagnosis," New England Journal of Medicine366, no. 14 (2012): 1310-1318, https://pubmed.ncbi.nlm.nih.gov/22475594/.
Donghao Lu et al., "Clinical diagnosis of mental disorders immediately before and after cancer diagnosis," JAMA Oncology 2, no. 9 (2016): 1188-1196, https://pubmed.ncbi.nlm.nih.gov/27124325/.
Neill Lambert et al., "Quantum biology," Nature Physics 9 (2013): 10-18, https://www.nature.com/articles/nphys2474.
Ron Sender, Shai Fuchs, and Ron Milo, "Revised estimates for the number of human and bacteria cells in the body," PLoS Biology 14, no. 8 (2016): e1002533, https://pubmed.ncbi.nlm.nih.gov/27541692/.
Ming Zhong et al., "Incidence of Spontaneous Resorption of Lumbar Disc Herniation is High: A Meta-Analysis," Pain Physician 20, no. 1 (2017): E45-E52, https://pubmed.ncbi.nlm.nih.gov/28072796/.
Chun-Chieh Chiu et al., "The probability of spontaneous regression of lumbar herniated disc: a systematic review," Clinical Rehabilitation 29, no. 2 (2015): 184-195, https://pubmed.ncbi.nlm.nih.gov/25009200/.
Praveen K. Reddy, Satish Sathyanarayana, and Anil Nanda, "MRI-documented spontaneous regression of cervical disc herniation: a case report and review of the literature," Journal of the Louisiana State Medical Society 155, no. 2 (2003): 97-98, https://pubmed.ncbi.nlm.nih.gov/12778993/.
K. Mochida et al., "Regression of cervical disc herniation observed on magnetic resonance images," Spine 23, no. 9 (1998): 990-995, https://pubmed.ncbi.nlm.nih.gov/9589536/.
Davide Festi et al., "Expectant management of gallstone disease is a valid therapeutic approach in the majority of patients," Journal of Gastroenterology and Hepatology 25, no. 4 (2010): 719-724, https://pubmed.ncbi.nlm.nih.gov/20492328/.
David P. McCormick et al., "Nonsevere acute otitis media: a clinical trial comparing outcomes of watchful waiting versus immediate antibiotic treatment," Pediatrics 115, no. 6 (2005): 1455-1465, https://pubmed.ncbi.nlm.nih.gov/15930204/.
Peter C. Albertsen, James A. Hanley, and Jason Fine, "20-year outcomes following conservative management of clinically localized prostate cancer," JAMA 293, no. 17 (2005): 2095-2101, https://pubmed.ncbi.nlm.nih.gov/15870412/.
Robert J. Fitzgibbons Jr. et al., "Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial," JAMA 295, no. 3 (2006): 285-292, https://pubmed.ncbi.nlm.nih.gov/16418463/.
Judith Meza-Junco et al., "Spontaneous regression of hepatocellular carcinoma: a systematic review," Annals of Hepatology 6, no. 1 (2007): 66-69, https://pubmed.ncbi.nlm.nih.gov/17297433/.
P. Papageorgiou, A. Katsambas, and A. Chu, "Phototherapy with blue (415 nm) and red (660 nm) light in the treatment of acne vulgaris," British Journal of Dermatology 142, no. 5 (2000): 973-978, https://pubmed.ncbi.nlm.nih.gov/10809858/.
P. J. Pacy et al., "Comparison of the hypotensive and metabolic effects of metoprolol therapy with a high fibre, low sodium, low fat diet in hypertensive type 2 diabetic subjects," Diabetes Research 1, no. 4 (1984): 201-207, https://pubmed.ncbi.nlm.nih.gov/6099231/.
Xin-hua Fan et al., "Comparative observation on acupuncture-moxibustion and western medication for treatment of sudden deafness," Zhongguo Zhen Jiu 30, no. 7 (2010): 553-556, https://pubmed.ncbi.nlm.nih.gov/20942277/.
Gianni Allais et al., "Acupuncture in the prophylactic treatment of migraine without aura: a comparison with flunarizine," Headache 42, no. 9 (2002): 855-861, https://pubmed.ncbi.nlm.nih.gov/12390610/.
Wei Huang et al., "Characterizing acupuncture stimuli using brain imaging with FMRI--a systematic review and meta-analysis of the literature," PLoS One 7, no. 4 (2012): e32960, https://pubmed.ncbi.nlm.nih.gov/22496739/.
I. R. Sanderson et al., "Remission induced by an elemental diet in small bowel Crohn's disease," Archives of Disease in Childhood 62, no. 2 (1987): 123-127, https://pubmed.ncbi.nlm.nih.gov/3548602/.
S. Takagi et al., "Effectiveness of an 'half elemental diet' as maintenance therapy for Crohn's disease: A randomized-controlled trial," Alimentary Pharmacology & Therapeutics 24, no. 9 (2006): 1333-1340, https://pubmed.ncbi.nlm.nih.gov/17059514/.
Myung-Haeng Hur et al., "Aromatherapy massage on the abdomen for alleviating menstrual pain in high school girls: a preliminary controlled clinical study," Evidence-Based Complementary and Alternative Medicine 2012 (2012): 187163, https://pubmed.ncbi.nlm.nih.gov/21949670/.
Patrick Catoire et al., "Hypnosis versus diazepam for embryo transfer: a randomized controlled study," American Journal of Clinical Hypnosis 55, no. 4 (2013): 378-386, https://pubmed.ncbi.nlm.nih.gov/23724572/.
N. Janakiramaiah et al., "Antidepressant efficacy of Sudarshan Kriya Yoga (SKY) in melancholia: a randomized comparison with electroconvulsive therapy (ECT) and imipramine," Journal of Affective Disorders 57, no. 1-3 (2000): 255-259, https://pubmed.ncbi.nlm.nih.gov/10708840/.
Bum Jin Park et al., "The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): evidence from field experiments in 24 forests across Japan," Environmental Health and Preventive Medicine 15, no. 1 (2010): 18-26, https://pubmed.ncbi.nlm.nih.gov/19568835/.
Benjamin Ka Seng Thong, Soelaiman Ima-Nirwana, and Kok-Yong Chin, "Proton pump inhibitors and fracture risk: a review of current evidence and mechanisms involved," International Journal of Environmental Research and Public Health 16, no. 9 (2019): 1571, https://pubmed.ncbi.nlm.nih.gov/31060319/.
Willy Gomm et al., "Association of proton pump inhibitors with risk of dementia: a pharmacoepidemiological claims data analysis," JAMA Neurology 73, no. 4 (2016): 410-416, https://pubmed.ncbi.nlm.nih.gov/26882076/.
Benjamin Lazarus et al., "Proton pump inhibitor use and the risk of chronic kidney disease," JAMA Internal Medicine 176, no. 2 (2016): 238-246, https://pubmed.ncbi.nlm.nih.gov/26752337/.
Ka Shing Cheung et al., "Long-term proton pump inhibitors and risk of gastric cancer development after treatment for Helicobacter pylori: a population-based study," Gut 67, no. 1 (2018): 28-35, https://pubmed.ncbi.nlm.nih.gov/29089382/.
George B. Stefano et al., "Endogenous morphine: up-to-date review 2011," Folia Biologica 58, no. 2 (2012): 49-56, https://pubmed.ncbi.nlm.nih.gov/22578954/.
Natalie Terry and Kara Gross Margolis, "Serotonergic mechanisms regulating the GI tract: experimental evidence and therapeutic relevance," Handbook of Experimental Pharmacology 239 (2017): 319-342, https://pubmed.ncbi.nlm.nih.gov/28035530/.
Michael F. Holick, "Vitamin D deficiency," New England Journal of Medicine 357, no. 3 (2007): 266-281, https://pubmed.ncbi.nlm.nih.gov/17634462/.
Bente Klarlund Pedersen, "Muscle as a secretory organ," Comprehensive Physiology 3, no. 3 (2013): 1337-1362, https://pubmed.ncbi.nlm.nih.gov/23897689/.
Sigrid Breit et al., "Vagus nerve as modulator of the brain-gut axis in psychiatric and inflammatory disorders," Frontiers in Psychiatry 9 (2018): 44, https://pubmed.ncbi.nlm.nih.gov/29593576/.
Luana Colloca and Arthur J. Barsky, "Placebo and nocebo effects," New England Journal of Medicine 382, no. 6 (2020): 554-561, https://pubmed.ncbi.nlm.nih.gov/32023375/.
Karla Kerlikowske et al., "Outcomes of screening mammography by frequency, breast density, and postmenopausal hormone therapy," JAMA Internal Medicine 173, no. 9 (2013): 807-816, https://pubmed.ncbi.nlm.nih.gov/23552817/.
Irene Papanicolas, Liana R. Woskie, and Ashish K. Jha, "Health care spending in the United States and other high-income countries," JAMA 319, no. 10 (2018): 1024-1039, https://pubmed.ncbi.nlm.nih.gov/29536101/.
Dan Buettner and Sam Skemp, "Blue Zones: lessons from the world's longest lived," American Journal of Lifestyle Medicine 10, no. 5 (2016): 318-321, https://pubmed.ncbi.nlm.nih.gov/30202288/.
Yuki Ideno et al., "Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): a systematic review and meta-analysis," BMC Complementary and Alternative Medicine 17, no. 1 (2017): 409, https://pubmed.ncbi.nlm.nih.gov/28814305/.
Elisabeth Conradi and Stefan Brenke, "Evidence-based health resort medicine," Forschende Komplementärmedizin22, no. 5 (2015): 324-333, https://pubmed.ncbi.nlm.nih.gov/26636026/.
No hay comentarios:
Publicar un comentario