Aug 19, 2025

When a Harvard-trained physician resorts to name-calling instead of scientific debate, you know you've struck a nerve. Dr. David Gorski's recent attack on my article "The FDA's War on Natural Thyroid: A Medical Tyranny That Threatens Millions" reads less like scientific criticism and more like a pharmaceutical industry hit piece disguised as medical commentary. His dismissive mockery of established biochemical principles, coupled with guilt-by-association fallacies and personal attacks, reveals the intellectual poverty of a medical establishment that has forgotten its primary obligation: to heal patients, not protect corporate profits.
The FDA's War on Natural Thyroid: A Medical Tyranny That Threatens Millions

Read, comment and PLEASE SHARE the X post dedicated to this article and call to action: https://x.com/sayerjigmi/status/1956722425493643308
Gorski's piece, published on Science-Based Medicine under the provocative title "What do mRNA vaccines, Synthroid, and pharmaceuticals have in common (according to MAHA)?", attempts to link legitimate concerns about natural thyroid therapy to anti-vaccine sentiment and political movements.¹ This guilt-by-association strategy represents the last refuge of those who cannot address the substance of scientific arguments. When peer-reviewed research contradicts pharmaceutical orthodoxy, apparently the appropriate response is character assassination rather than scientific refutation.
The stakes in this debate extend far beyond thyroid therapy. At issue is whether patients retain fundamental autonomy over their medical decisions, or whether a captured regulatory apparatus can force millions into a one-size-fits-all pharmaceutical paradigm that enriches corporations while ignoring documented patient suffering. Gorski's position perfectly aligns with an industry that profits from restricting access to effective, non-patentable treatments—a coincidence too convenient to ignore.
The Regulatory Context: A Critical Transition Moment
[FDA Update (August 17, 2025): The FDA has moved Armour, NP, and all natural thyroid medicines into the "unapproved drug" category. This classification doesn't mean unsafe—many patients have relied on these treatments for decades—but it does create stigma and uncertainty around access.]
It's crucial to understand what this regulatory designation actually means versus what it appears to suggest. The "unapproved" status represents a bureaucratic technicality, not a safety determination. These products have maintained exemplary safety records spanning over 130 years of clinical use. The FDA's own adverse event databases show remarkably low complication rates for DTE compared to synthetic alternatives.
Dr. Marty Makary's stated commitment to pursue the first-ever formal approval of DTE through clinical trials offers hope, but until approval is achieved, every current DTE product remains in a vulnerable regulatory position.² This transition period requires unprecedented vigilance from patients, physicians, and advocates to ensure continued access to effective treatments.
Patients deserve clarity and continuity, not regulatory uncertainty that creates barriers to established therapies. This moment should be seen as an opportunity to formalize the scientific evidence supporting natural thyroid through rigorous trials, while maintaining access for the millions who depend on these treatments for their health and quality of life.
The Clinical Evidence Gorski Conveniently Ignored
Rather than engage with the substantial body of peer-reviewed research supporting natural desiccated thyroid extract (DTE), Gorski cherry-picks arguments while ignoring the most compelling clinical data. This selective blindness to inconvenient evidence reveals the weakness of his position.

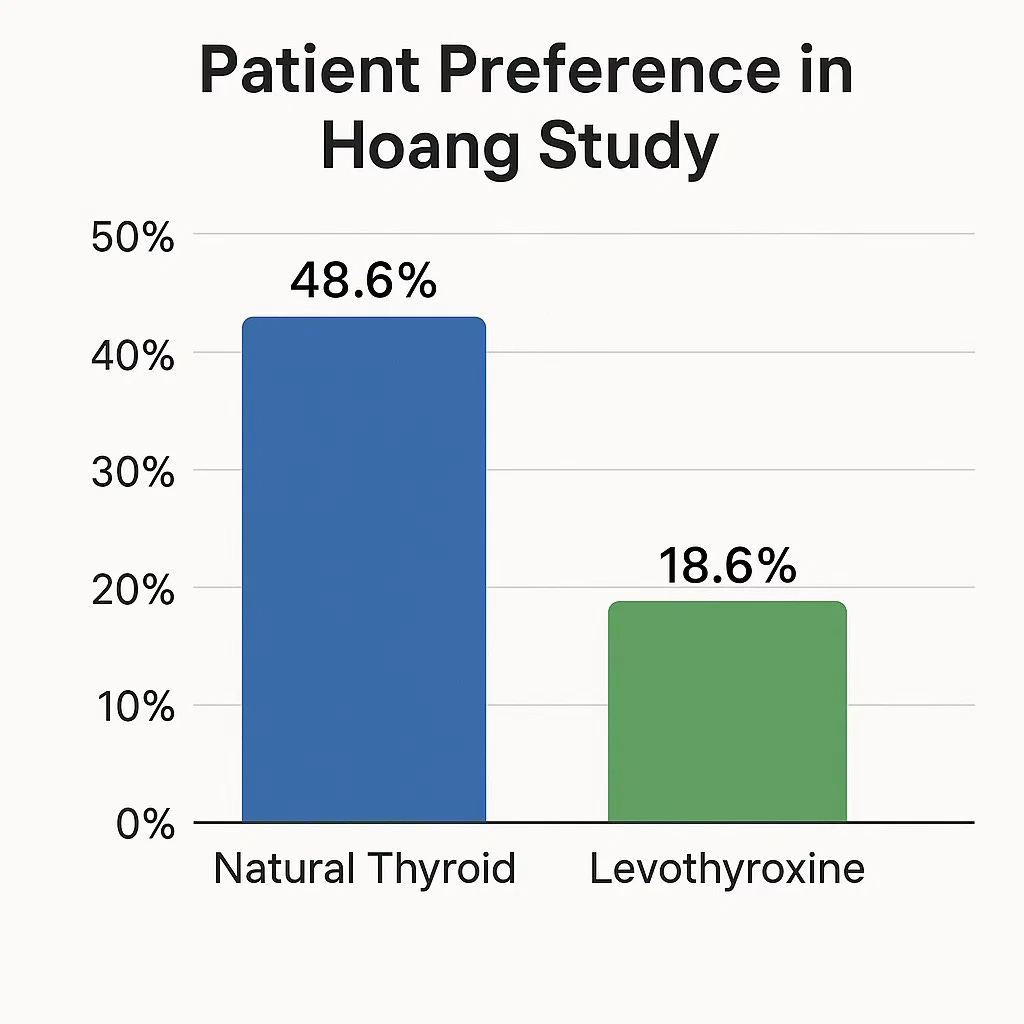
The landmark 2013 Hoang study in the Journal of Clinical Endocrinology & Metabolism demonstrated that nearly three times as many patients preferred natural thyroid over synthetic levothyroxine when given the choice in a randomized, double-blind crossover trial (48.6% vs 18.6%).³ These weren't subjective impressions—patients on DTE experienced statistically significant weight loss (3-4 pounds), improved energy levels, and better quality of life scores compared to synthetic T4. The weight loss alone provides objective evidence of improved metabolic function, contradicting any claims of placebo effect.
The 2021 Shakir study reinforced these findings with even more compelling data. Among patients who remained symptomatic on standard T4 therapy—those failed most dramatically by the synthetic approach—fully one-third experienced significant improvements when switched to treatments containing T3, whether DTE or synthetic combinations.⁴ These patients showed marked improvements in symptom scores, mood measures, and cognitive function. When a third of treatment-resistant patients find relief with natural thyroid, dismissing this as irrelevant becomes medical malpractice.
Gorski acknowledges these studies exist but minimizes their significance, claiming that "average outcomes" were similar across therapies. This statistical sleight of hand obscures the crucial finding: while many patients do fine on T4 alone, a substantial minority—estimated at 10-15% of all hypothyroid patients—cannot efficiently convert T4 to active T3 due to genetic polymorphisms affecting deiodinase enzymes.⁵ For these millions, synthetic levothyroxine represents suboptimal therapy, flooding their bodies with inactive storage hormone while providing insufficient active T3 for optimal tissue function.
The Molecular Reality Gorski Cannot Refute
Gorski's most revealing moment comes when he ridicules established biochemical concepts like hydration shells, protein conformational dynamics, and structured water environments. His mockery exposes a fundamental misunderstanding of modern molecular biology. These aren't mystical concepts—they represent the cutting edge of our understanding of how biological systems actually function.
Every biomolecule in living systems exists within a structured hydration shell—ordered water molecules that interact with and influence molecular behavior. This is mainstream biochemistry, documented in prestigious journals like Chemical Reviews.⁶ Water in the immediate vicinity of proteins has distinct ordering compared to bulk water, and this ordering helps maintain protein structure and function. To dismiss this as "homeopathy-adjacent" reveals either ignorance or intellectual dishonesty.
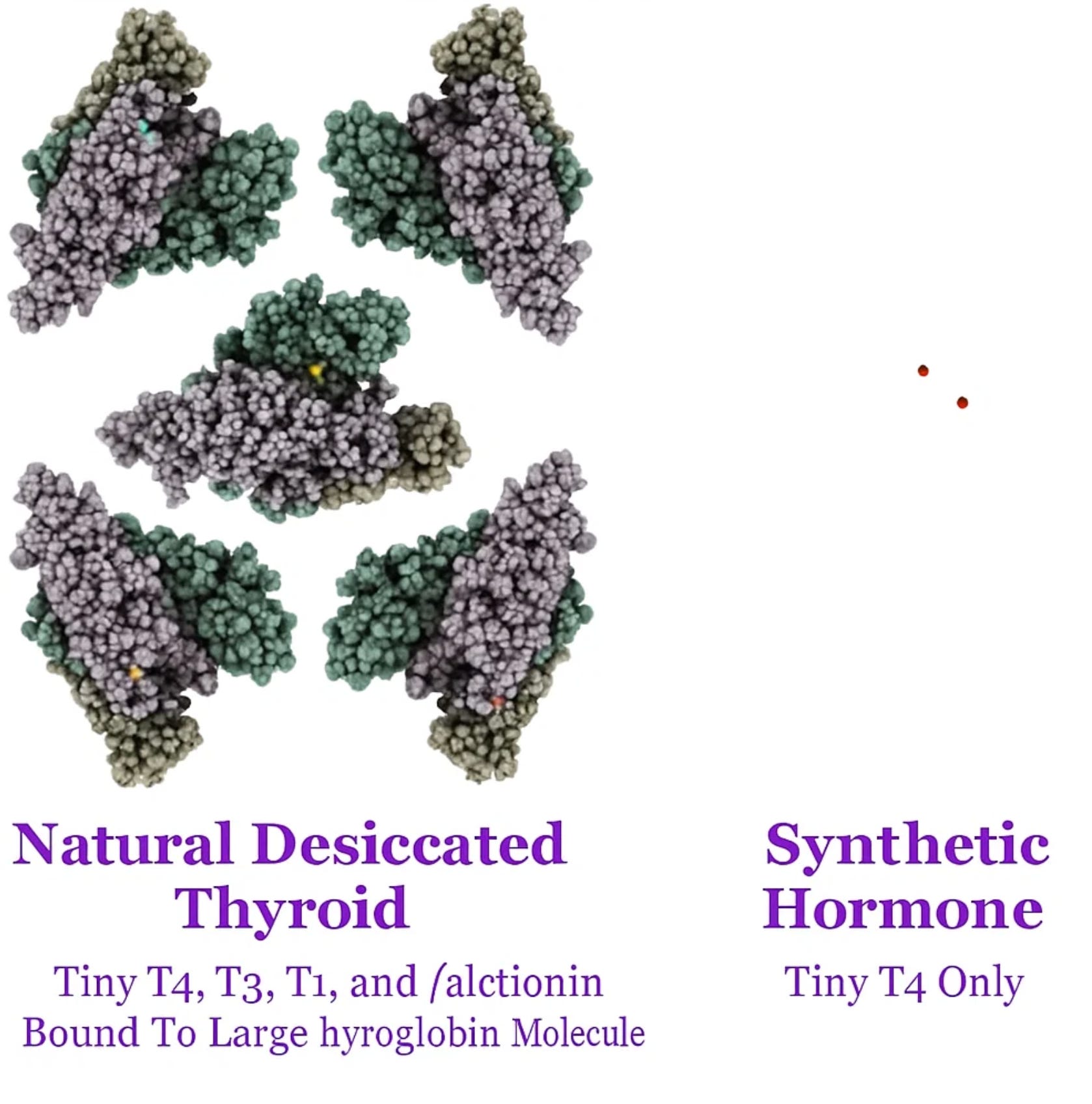
Natural desiccated thyroid delivers hormones within the evolutionary-optimized context of thyroglobulin—a massive 660,000 dalton protein complex that has spent millions of years perfecting hormone storage, transport, and release.⁷ Each T4 molecule exists in specific conformational states (simultaneously informational/functional states), held in precise spatial relationships that the body recognizes and processes efficiently. This isn't speculation—it's the result of detailed crystallographic and biochemical studies of thyroglobulin structure.
Synthetic levothyroxine, by contrast, consists of isolated molecules stripped of all biological context. These molecular entities must navigate the body's varying pH environments—from stomach acid (pH 1-2) to intestinal alkalinity (pH 7-8) to blood plasma (pH 7.4)—without the stabilizing matrix that nature provides. As they encounter different conditions, they can populate multiple rotameric states and ionization configurations, potentially creating highly variable biological activity.
This represents fundamental physical chemistry principles. The same concept explains why hemoglobin carries oxygen more effectively than isolated heme groups, or why insulin functions optimally in its native hexameric form (packaged with C-peptide) rather than as isolated monomers. Biological systems evolved sophisticated packaging for their active molecules, and understanding that packaging provides insights into optimal therapeutic delivery.
Addressing the "Consistency" Argument: The Deeper Molecular Truth
One of the most sophisticated arguments against natural thyroid involves claims about dosing consistency. A recent reader comment exemplifies this thinking: "The problem with natural Armour thyroid is that it's very difficult to maintain the same exact dose because every pig is different. As a result the TSH levels can dramatically change, which is not healthy."
This argument fundamentally misunderstands both the nature of biological medicines and the molecular reality of what "consistency" actually means. Let's examine why this reasoning not only misses the mark but actually inverts the truth about therapeutic reliability.
The Rotameric and Ionization Reality
When defenders of synthetic thyroid claim superior "consistency," they make a critical error: they assume that identical chemical mass equals identical biological activity. Modern molecular biology reveals that the same molecule can exist in multiple rotameric states (different three-dimensional orientations) and varying ionization states (different electrical charges) depending on its environment.
Consider what happens with synthetic levothyroxine like Tirosint as it travels through the body:
In stomach acid (pH 1-2): The molecule exists in one ionization state
In small intestine (pH 7-8): It shifts to another configuration
In blood plasma (pH 7.4): It adopts yet another form
At cellular membranes: Further conformational changes may occur
Each of these states represents a functionally different form of the "same" molecule. The synthetic hormone, lacking the biological scaffolding that natural thyroid provides, becomes more susceptible to these environmental variations because it has no organizing matrix to provide stability.
Keep in mind that the process by which levothyroxine sodium is produced today is highly synthetic and involves the use of a wide range of chemicals. One patent describes the dizzyingly complex process as follows:
"The process for preparation of Levothyroxine sodium comprises the steps, wherein compound obtained from steps a-g is prepared by conventional methods, a. nitrating L-tyrosine to give 3,5- dinitro-L-tyrosine, b. acetylating 3,5- dinitro-L-tyrosine to give 3,5- dinitro-N-acetyl L-tyrosine, c. esterifying the compound obtained from step (b) to give 3,5- diπitro-N-acetyl L-tyrosine ethyl ester, d. reacting the compound obtained from step (c) with p-TsCI in presence of pyridine to give corresponding tosylate salt, which is further reacting with 4-methoxy phenol to give 3,5- DinKro-4-p-methoxy phenoxy-N-acetyl-L-phenyl alanine ethyl ester, e. the compound obtained from step (d) is hydrogenated to give 3,5-diamino-4-p-methoxy phenoxy-N-acetyl-L-phenyl alanine ethyl ester, f. the compound obtained from step (e) is tetrazotized and iodized to give 3,5-Diiodo-4-p- methoxy phenoxy-N-acetyl-L-phenyl alanine ethyl ester, g. the compound obtained from step (f) is O-demethylated, N-deacetylated, and deesterified using aqueous HI in acetic acid to give 3,5-Diiodo-4-p-hydroxy phenoxy-L-pheπyl alanine followed by preparing hydrochloride salt of same and isolating, drying it h. lodinating 3,5-Diiodo-4-p-hydroxy pheπoxy-L-phenyl alanine HCI salt using methyl amine.”
Consider this profound juxtaposition: the infinite intelligence of biological systems evolved over millions of years versus the reductionist hubris of industrial chemistry. Which do you trust will serve your physiology better—a hormone delivered within its evolutionary context, or an isolated chemical fragment manufactured in industrial reactors?
The answer becomes self-evident when we honor biological intelligence over pharmaceutical reductionism.
This explains why patients consistently report transformative results with natural thyroid extract. Their bodies recognize and respond to complete biological information encoded within naturally-derived hormones.
No amount of pharmaceutical-industry-aligned medical gaslighting by physicians like Gorski can alter this fundamental reality: you are the ultimate authority on your own biological experience. Your N-of-1—your individual response, your quality of life, your energy—carries infinitely more relevance for your health than any clinical trial you never participated in.
Your body's wisdom transcends statistical abstractions. When millions report superior outcomes with natural thyroid, they're demonstrating the superior intelligence of biological systems over pharmaceutical approximations.
Trust your experience. Trust your body's evolutionary wisdom. That represents true science-based medicine.
The Manufacturing Reality: Data Versus Perception
The claim about "every pig being different" ignores the sophisticated pharmaceutical standards governing modern natural thyroid manufacturing:
FDA requires 95-105% potency for all thyroid medications, natural and synthetic
Each batch undergoes biological assays for T4 and T3 content verification
Modern manufacturing pools thyroid tissue from thousands of animals, effectively averaging out individual variations
Quality control testing ensures consistent hormone levels across production batches
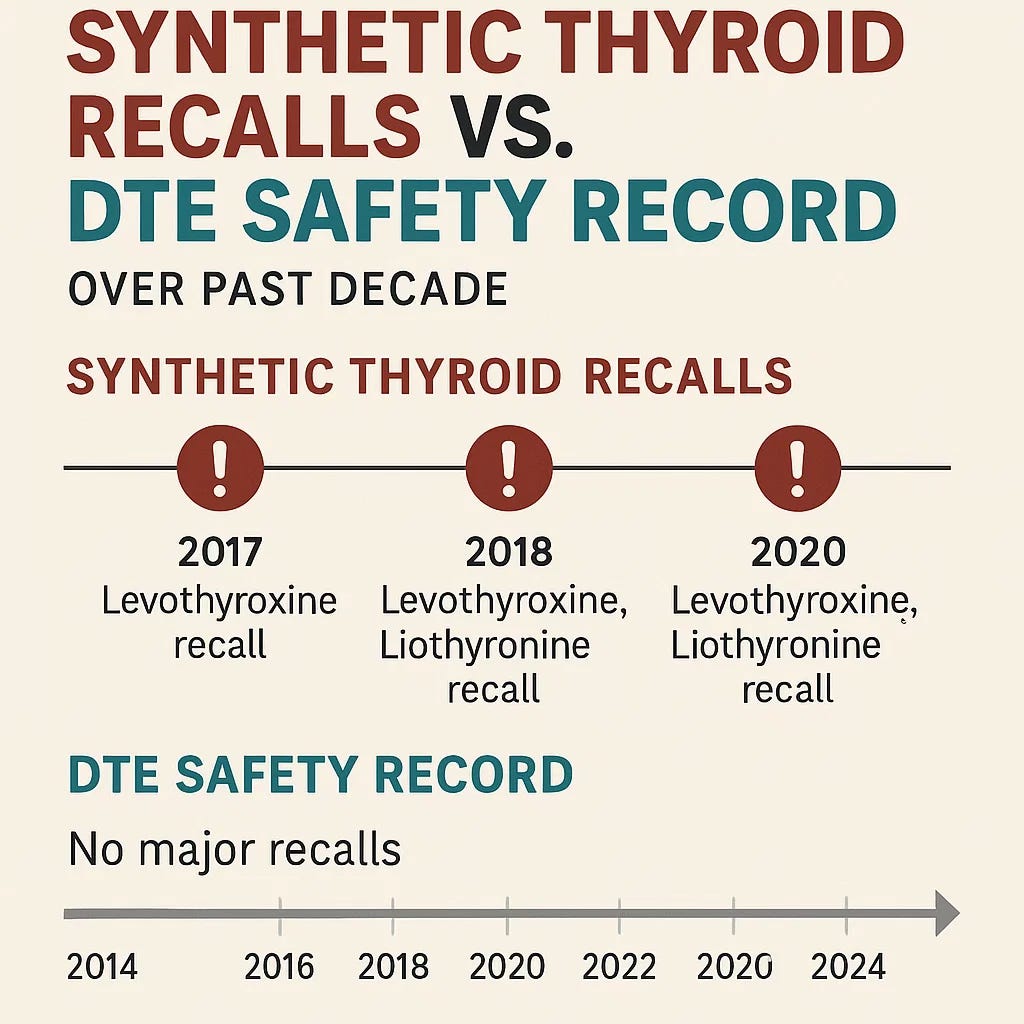
Meanwhile, synthetic levothyroxine's actual consistency record reveals significant challenges:
Over 160,000 bottles recalled in 2025 for failing potency specifications⁸
Multiple recalls across different manufacturers for both super-potency and sub-potency issues
Documented degradation with heat and humidity exposure
Tablet-to-tablet variation documented within single bottles
The TSH Obsession: Missing the Forest for the Trees
The fixation on maintaining perfectly stable TSH levels represents perhaps the greatest conceptual error in modern thyroid management. This approach mistakes the map for the territory, focusing on a single laboratory value rather than comprehensive patient wellness.
TSH is a pituitary hormone, not a thyroid hormone—it reflects what the pituitary gland wants, not necessarily what peripheral tissues are receiving. Many patients maintain "optimal" TSH levels while experiencing persistent hypothyroid symptoms, a phenomenon that synthetic-only advocates struggle to explain.
Natural thyroid's minor TSH variations may actually represent healthier physiology:
Physiologic thyroid output naturally varies throughout circadian cycles
Rigid TSH stability is artificial and potentially suboptimal
Natural fluctuations may better match evolutionary hormone patterns
Multiple hormone pathways provide functional redundancy
True Consistency: Functional Versus Chemical
When we examine the deeper molecular reality, natural thyroid provides several forms of consistency that synthetic hormones cannot match:
Conformational Consistency: Hormones held within evolved protein scaffolding that buffers environmental changes
Functional Consistency: Multiple hormone pathways ensuring therapeutic effect even if individual conversion processes vary
Evolutionary Consistency: Hormone presentation matching what human physiology evolved to recognize
Therapeutic Consistency: Superior patient outcomes documented in controlled trials
Synthetic T4, while chemically uniform, actually provides:
Chemical consistency that ignores biological complexity
Rotameric variability without biological guidance
Ionization instability across body compartments
Therapeutic inconsistency evidenced by millions of symptomatic patients
The Economics of Medical Control
Gorski's position becomes even more suspect when viewed through the lens of economic incentives driving this manufactured crisis. The global levothyroxine market generates over $4 billion annually, projected to reach nearly $6 billion by 2033.⁹ Synthetic T4 costs dramatically less to produce than natural thyroid extract, yet commands similar prices—creating substantial profit margins that natural alternatives directly threaten.

The pharmaceutical industry's business model depends on patentable synthetic molecules that can be sold at controlled prices. Natural thyroid extract represents a fundamental challenge to this paradigm—it's a non-patentable treatment derived from biological sources that patients often prefer and that demonstrates superior outcomes for many individuals.
Consider the key players: AbbVie, the pharmaceutical corporation behind both Synthroid and Armour Thyroid, has invested millions in lobbying efforts.¹⁰ While smaller DTE manufacturers face regulatory pressure, AbbVie's products remain protected through the transition period. This selective treatment reveals the true dynamics—not patient safety, but market control.
Research demonstrates that 73% of FDA advisory meetings include members with pharmaceutical industry financial ties.¹¹ When the agency responsible for protecting public health includes individuals with economic stakes in pharmaceutical companies, regulatory capture becomes virtually inevitable.
Food as Medicine: The Paradigm Under Siege
Natural desiccated thyroid represents something far more threatening to pharmaceutical interests than just another treatment option—it embodies the fundamental principle of food as medicine. DTE is essentially concentrated organ meat, the same thyroid tissue that traditional cultures valued for its health-promoting properties. For over 130 years, this straightforward approach has successfully managed hypothyroidism.
The pharmaceutical industry's opposition to food-based medicine extends beyond mere competition—it challenges their core business model. Natural substances cannot be patented. Biological materials cannot command monopoly pricing. The existence of effective natural treatments undermines the industry's central narrative that synthetic chemicals represent superior therapy.
This explains the systematic campaign against traditional medicine approaches, from restrictions on herbal treatments to regulatory barriers for nutritional therapies. Each success in eliminating natural alternatives strengthens pharmaceutical market control, forcing patients into dependence on patentable synthetic substitutes regardless of their comparative effectiveness or safety profiles.
The FDA's current action against natural thyroid establishes a concerning precedent. If successful, this regulatory framework will likely be applied to other natural treatments—bioidentical hormones, nutritional supplements, compounded medications, and any therapy that competes with pharmaceutical revenues.
Deconstructing Gorski's Intellectual Approach
Gorski's critique employs several argumentative strategies that merit examination:
Guilt by Association: Rather than address the scientific merits of natural thyroid therapy directly, Gorski attempts to discredit it by linking advocates to unrelated political movements. This approach substitutes character evaluation for scientific argument.
Appeal to Institutional Authority: Gorski repeatedly cites American Thyroid Association and FDA positions as definitive evidence. Authentic scientific evaluation examines evidence on its merits, not the institutional status of those making claims.
Selective Evidence Presentation: Gorski misrepresents the molecular arguments for natural thyroid, reducing sophisticated biochemical concepts to simplified versions he can more easily challenge. This technique avoids engaging with the actual scientific evidence in its full complexity.
Patient Experience Dismissal: Throughout his analysis, Gorski minimizes patient-reported outcomes rather than investigating why patients report better results with natural thyroid. When thousands of patients report improvements validated by controlled trials, dismissing these experiences contradicts patient-centered medicine principles.
The most concerning aspect of Gorski's approach involves his treatment of patient experiences as inherently unreliable. When substantial numbers of patients report life-changing improvements on natural thyroid, and controlled trials validate these reports, dismissing patient voices represents a fundamental misunderstanding of medicine's purpose.
The Postmenopausal Population: A Case Study in Treatment Individualization
One of the most significant gaps in synthetic-only approaches involves the systematic undertreatment of postmenopausal women. Research demonstrates that declining estrogen levels directly impair the body's ability to convert T4 to active T3, yet standard protocols continue prescribing T4-only treatment for this vulnerable population.¹²
This demographic faces multiple converging challenges:
Estrogen decline reduces T4-to-T3 conversion efficiency
Age-related decreases in deiodinase enzyme activity
Increased osteoporosis risk from hormonal deficiencies
Higher rates of cardiovascular and cognitive complications
Natural thyroid extract provides these women with direct T3 to circumvent conversion limitations and calcitonin to support bone health—benefits that synthetic T4 monotherapy cannot deliver. Studies indicate that 50% of thyroidectomized patients develop osteopenia specifically from calcitonin deficiency.¹³ Moreover, there are a wide range of natural approaches to addressing hypothyroidism and the root-case resolution layer of the problem. You can consult the GreenMedInfo.com database to learn more.

Clinical evidence demonstrates that postmenopausal women on natural thyroid experience:
Enhanced cognitive function and mental clarity
Improved energy levels and reduced fatigue
Modest but significant weight management benefits
Better mood stability and reduced depression symptoms
Improved bone density maintenance
The medical establishment's reluctance to acknowledge these benefits represents a significant gap in women's healthcare.
The Safety Record: Evidence-Based Risk Assessment
Gorski's safety arguments require careful examination against actual evidence. Natural thyroid extract maintains the longest documented safety record of any thyroid medication, spanning 130 years with minimal serious adverse events. During this period, it transformed myxedema from a universally fatal condition to a manageable disorder.
The FDA's own adverse event database provides important context. Between 1968-2025, only 500 adverse events were reported for DTE—approximately nine per year across millions of patient exposures.¹⁴ This compares favorably to synthetic levothyroxine's profile:
Documented associations with increased cardiovascular risks in certain populations¹⁵
Links to bone density issues from over-replacement¹⁶
Multiple manufacturing failures and product recalls
Higher adverse event rates when adjusted for usage patterns
Independent analysis of FDA adverse event databases suggests that synthetic medications may have proportionally higher rates of certain complications than natural thyroid preparations, even accounting for the larger user population.¹⁷ This evidence contradicts claims that synthetic options are inherently safer.
The agency's differential enforcement patterns raise additional questions. Smaller natural thyroid manufacturers face significant regulatory scrutiny for minor potency variations, while major pharmaceutical companies continue operations despite quality control issues. This inconsistent application of standards suggests factors beyond pure safety considerations.
The Path Forward: Preserving Medical Choice
The resolution to this controversy lies not in eliminating either natural or synthetic thyroid options, but in defending the fundamental principle that both should remain available for patients who benefit from them. Optimal medical practice occurs when physicians can individualize treatment based on patient response, genetic factors, and clinical judgment rather than regulatory restrictions serving narrow interests.
Essential Actions for Protecting Patient Choice:
Legislative Advocacy: Support the Thyroid Disease CARE Act (H.R.10297) that specifically addresses barriers to accessing diverse thyroid treatments.¹⁸ Congressional oversight becomes crucial when regulatory agencies may prioritize industry interests over patient welfare.
Legal Protection: The evolving legal landscape offers opportunities to challenge arbitrary regulatory restrictions. Courts increasingly evaluate agency actions on their scientific merits rather than automatically deferring to bureaucratic authority.
Medical Education: Healthcare training programs should incorporate research supporting individualized thyroid therapy approaches. Physicians need comprehensive knowledge to make evidence-based decisions rather than following pharmaceutical marketing presentations disguised as clinical guidelines.
Patient Empowerment: The most influential force for positive change remains informed patients advocating for treatments that improve their health and quality of life. When millions of Americans share their success experiences with natural thyroid, regulatory agencies cannot indefinitely ignore this feedback.
Research Support: Funding for comparative effectiveness research examining different thyroid therapy approaches will provide additional evidence for personalized treatment decisions.
Beyond Replacement Therapy: The Root Cause Revolution
While this debate centers on natural versus synthetic thyroid replacement, a far more crucial conversation remains systematically ignored by the medical establishment: Why are millions developing thyroid dysfunction in the first place? The pharmaceutical paradigm profits from treating symptoms while ignoring the environmental and nutritional factors creating epidemic thyroid disease.
The Preventable Epidemic
The tragic irony of modern thyroid medicine lies not just in restricting access to effective treatments, but in the systematic creation of thyroid disease through:
Iodine Deficiency Crisis: Despite fluoridated water and iodized salt, over 90% of Americans remain iodine deficient according to WHO standards. The average American consumes less than half the minimum daily requirement, creating widespread subclinical hypothyroidism that conventional medicine either misses or mismanages.
Selenium Depletion: Industrial agriculture has stripped selenium from soils across vast regions. This essential mineral serves as the rate-limiting cofactor for thyroid hormone conversion—without adequate selenium, even optimal T4 levels cannot generate sufficient active T3. Yet standard thyroid panels never assess selenium status.
Halogen Class Endocrine Disruptors: Fluoride in water supplies, brominated flame retardants in furniture, and chlorinated compounds in household products systematically block iodine uptake at cellular receptors. These halogen disruptors create functional iodine deficiency even when dietary intake appears adequate.
Goitrogenic Food Exposures: Unfermented soy products, excessive raw cruciferous vegetables, and industrial food additives contain compounds that actively suppress thyroid function. Most patients receive zero nutritional counseling about foods that may be sabotaging their thyroid health.
Diagnostic Overreach and Overtreatment: Perhaps the greatest tragedy involves the systematic destruction of healthy thyroid tissue through unnecessary biopsies, radioactive iodine treatments, and surgical interventions. The current diagnostic paradigm creates thyroid patients where none existed, transforming minor nodules and subclinical variations into medical emergencies requiring permanent pharmaceutical dependency.
Root Cause Medicine: Addressing the WHY
True healing begins by asking why thyroid dysfunction develops, not just what synthetic or natural molecule can replace missing function, or even feed a deficiency that causes greater gland atrophy. Root cause medicine offers a fundamentally different approach:
Nutritional Restoration: Comprehensive assessment and correction of iodine, selenium, zinc, tyrosine, and B-vitamin deficiencies that enable optimal thyroid function. Many patients experience dramatic improvements simply by addressing nutritional foundations that conventional medicine ignores.
Environmental Detoxification: Systematic reduction of halogen exposures, heavy metal burdens, and endocrine-disrupting chemicals that interfere with thyroid physiology. This includes water filtration, organic food choices, and safer household products.
Dietary Optimization: Elimination of goitrogenic foods during healing phases, incorporation of thyroid-supportive nutrients, and restoration of gut health that enables proper hormone absorption and conversion.
Stress Management: Chronic stress elevates cortisol, which directly suppresses T4-to-T3 conversion and TSH production. Addressing psychological, physical, and biochemical stressors often restores normal thyroid function without pharmaceutical intervention.
Microbiome Restoration: Emerging research demonstrates that gut bacteria play crucial roles in thyroid hormone metabolism. Antibiotic damage, processed food consumption, and inadequate fiber intake create dysbiosis that impairs thyroid function.
The GreenMedInfo.com database contains over 100,000+ peer-reviewed studies documenting natural approaches to health, many of which are relevant to thyroid disease—evidence that the medical establishment systematically ignores in favor of pharmaceutical solutions.
Prevention Before Dependency
The most profound medical intervention involves preventing thyroid disease before permanent damage occurs. This requires:
Early Nutritional Assessment: Testing and optimizing iodine, selenium, and cofactor status before subclinical deficiencies progress to overt disease.
Environmental Awareness: Education about thyroid-disrupting exposures and practical steps to minimize them in daily life.
Dietary Education: Understanding how food choices directly impact thyroid function, both positively and negatively.
Diagnostic Restraint: Avoiding unnecessary interventions for minor thyroid variations that may resolve with nutritional and environmental optimization.
Functional Medicine Approaches: Working with practitioners who understand root cause analysis rather than symptom suppression.
The Economic Reality of Prevention
The medical establishment's resistance to root cause approaches becomes clear when viewed through economic incentives. A patient whose thyroid dysfunction resolves through nutritional optimization generates no ongoing pharmaceutical revenue. Someone whose environmental toxic load decreases requires fewer medical interventions. Individuals who maintain optimal thyroid function through lifestyle choices need no prescription medications.
Conversely, patients dependent on synthetic thyroid replacement generate consistent revenue streams for decades. The current system profits from creating and maintaining disease, not preventing or curing it.
This explains why medical schools provide minimal nutrition education, why environmental toxicity receives little attention in clinical practice, and why root cause approaches remain marginalized despite overwhelming scientific support.
Reclaiming Thyroid Health
For those already dependent on thyroid replacement therapy, natural desiccated thyroid offers superior outcomes as documented throughout this article. But for the millions developing subclinical dysfunction, early intervention with root cause medicine may prevent the need for any pharmaceutical dependency.
Your thyroid wasn't designed to fail. It's responding to environmental insults, nutritional deficiencies, and toxic exposures that the medical system ignores while profiting from the resulting disease. Understanding and addressing these root causes represents the ultimate expression of medical freedom—preventing disease rather than managing pharmaceutical dependency.
The choice extends beyond natural versus synthetic thyroid replacement. The choice involves reclaiming health through biological intelligence rather than accepting pharmaceutical dependency as inevitable.
The Broader Context: Medical Freedom Versus Corporate Control
This debate over thyroid therapy represents a critical test case for the future direction of American healthcare. The fundamental question is whether we maintain a system that honors patient choice, physician judgment, and scientific evidence, or whether we accept pharmaceutical industry control over treatment options regardless of patient outcomes.
Gorski's position—reflecting much of the medical establishment—represents a worldview that prioritizes pharmaceutical industry interests over patient welfare, regulatory convenience over medical freedom, and corporate profits over individual health outcomes. His intellectual approach, reliance on argumentative techniques that avoid evidence, and dismissal of patient experiences reveal concerning trends in modern medical discourse.
The evidence supporting natural thyroid therapy continues strengthening:
Multiple peer-reviewed studies demonstrate superior patient outcomes for significant subgroups
Genetic research validates the clinical need for T3-containing therapies
Molecular biology provides mechanistic explanations for biological complexity benefits
Clinical experience confirms that individualized approaches produce better results
Patient preferences remain clear and consistent:
Nearly 3:1 preference for natural thyroid in controlled trials
Significant improvements in quality of life measures
Objective metabolic improvements including weight management
Superior outcomes for patients who respond poorly to synthetic-only treatment
The safety profile spans over a century without major incidents:
Minimal adverse events in regulatory databases
Favorable complication rates compared to synthetic alternatives
Successful use in millions of patients worldwide
No documented safety signals requiring access restrictions
The primary arguments against natural thyroid originate from regulatory agencies and pharmaceutical industry representatives whose economic interests align with restricting patient choice. Their positions contradict scientific evidence, patient preferences, clinical experience, and the fundamental principles that should guide ethical medical practice.
Conclusion: Defending Science-Based Medicine
Dr. Gorski's attack on natural thyroid advocates represents more than academic disagreement—it exemplifies a captured medical establishment's effort to protect pharmaceutical industry profits while dismissing patient welfare. His resort to personal attacks, logical fallacies, and intellectual dismissiveness reveals the fundamental weakness of the synthetic-only position.
When prominent physicians abandon scientific discourse in favor of character attacks, we witness the corruption of medical institutions by commercial interests. When regulatory agencies ignore decades of safety data to advance corporate agendas, we observe the complete capture of public health systems by private industry.
The millions of Americans who depend on natural thyroid therapy deserve evidence-based healthcare decisions rather than bureaucratic restrictions disguised as scientific authority. Their health outcomes, their treatment choices, their right to therapies that improve their lives—these principles transcend political boundaries and economic interests. They represent the foundational values upon which ethical medicine must operate.
In defending natural thyroid therapy, we defend something more fundamental: the human right to medical treatments that enhance health and quality of life. This struggle will determine whether medicine serves patients or corporations, whether science guides practice or profits dictate policy, whether physicians heal individuals or enforce pharmaceutical industry preferences.
The regulatory transition period we're currently experiencing requires unprecedented vigilance from patients, advocates, and healthcare providers to ensure continued access to effective treatments while formal approval processes proceed. Dr. Makary's commitment to pursuing official DTE approval through clinical trials provides hope, but patients cannot afford interruptions in access to treatments that have safely and effectively served them for over a century.
The scientific evidence is comprehensive. The patient preference data is clear. The safety record is exemplary. The choice remains ours.
This moment will define whether American medicine advances toward personalized, evidence-based care that honors individual patient needs, or retreats into a pharmaceutical monoculture that prioritizes industry profits over human health. The millions who benefit from natural thyroid therapy deserve nothing less than our strongest advocacy for their continued access to effective treatment.
References:
Gorski, D. "What do mRNA vaccines, Synthroid, and pharmaceuticals have in common (according to MAHA)?" Science-Based Medicine, August 18, 2025.
Makary, M. [@DrMakaryFDA]. "FDA is committed to pursuing the first-ever approval of desiccated thyroid extract, pending results of the ongoing clinical trials." Twitter, August 13, 2025.
Hoang TD, et al. "Desiccated thyroid extract compared with levothyroxine in the treatment of hypothyroidism: a randomized, double-blind, crossover study." J Clin Endocrinol Metab. 2013;98(5):1982-1990.
Shakir MKM, et al. "Comparative effectiveness of levothyroxine, desiccated thyroid extract, and levothyroxine+liothyronine in hypothyroidism." J Clin Endocrinol Metab. 2021;106(11):e4400-e4413.
Peterson SJ, et al. "Levothyroxine monotherapy cannot guarantee euthyroidism in all athyreotic patients." J Clin Endocrinol Metab. 2016;101(12):4964-4973.
Laage D, et al. "Water dynamics in the hydration shells of biomolecules." Chem Rev. 2017;117(16):10694-10725.
Coscia F, et al. "Formation of thyroid hormone revealed by a cryo-EM structure of native bovine thyroglobulin." Nature Communications. 2022;13:2261.
FDA Recall Notice. "Levothyroxine sodium tablets recalled for subpotency." July 2025.
Business Research Insights. "Levothyroxine Market Analysis 2024-2033." Market Research Report, 2024.
OpenSecrets.org. "AbbVie Inc Lobbying Profile." 2024.
Pham-Kanter G. "Revisiting financial conflicts of interest in FDA advisory committees." Milbank Q. 2014;92(3):446-470.
Santin AP, et al. "Increased serum interleukin-6 is predictive of thyroid dysfunction in postmenopausal women." J Endocrinol Invest. 2007;30(6):489-496.
Lakatos P, et al. "Thyroidectomy-induced calcitonin deficiency and osteopenia." Bone. 1991;12(6):397-402.
FDA FAERS Database. "Adverse event reports for desiccated thyroid extract, 1968-2025."
Biondi B, et al. "Cardiovascular effects of mild hypothyroidism." Thyroid. 2007;17(7):625-630.
Brennan MD, et al. "Bone mineral density in hypothyroid patients treated with levothyroxine." Arch Intern Med. 1988;148(4):809-811.
OpenVAERS Analysis. "Comparative adverse event rates: DTE vs synthetic levothyroxine." August 2025.
H.R.10297. "Thyroid Disease CARE Act of 2024." 118th Congress.
No hay comentarios:
Publicar un comentario