Sayer Ji
Sep 18, 2025

Key Points:
Minimal Infant Risk: Hepatitis B primarily spreads through sex or blood contact; healthy newborns of HBV-negative mothers face near-zero infection risk, calling into question routine vaccination at birth².
Documented Harms: Over 100 studies link the HepB vaccine to serious adverse outcomes, including autoimmune diseases, neurological damage, liver injury, and systemic inflammation⁵⁶⁷⁸. Ironically, a shot meant to protect the liver can cause liver cell death and dysfunction³⁴.
Efficacy Gaps: Producing antibodies ≠ lasting immunity. Even “fully vaccinated” individuals can contract hepatitis B or harbor silent (occult) infections¹⁴⁶. In fact, immunity from an infant HepB shot may vanish by young adulthood – just when hepatitis exposure becomes relevant³¹⁶.
Paradigm Shift: Emerging research on exosomes (cellular particles akin to viruses) suggests hepatitis B might stem more from toxins than germs. This “poisoned-not-infected” perspective challenges germ theory and urges a move away from one-size-fits-all vaccination dogma toward biologically grounded, individualized health strategies¹⁵¹⁶.
On the eve of ACIP’s vote on hepatitis B vaccination, one question towers above the talking points: why are we injecting 100% of newborns for a condition that ~0% of HBV-negative mothers’ babies will face in early life? As the committee readies its decision, the public will hear familiar refrains—“safe and effective,” “lifesaving,” “settled science.” Yet the record shows something messier: occult infections despite full vaccination, waning protection by adolescence, aluminum-driven inflammation in the first 24 hours of life, and credible autoimmune/neurologic injury signals that never make it into the press release. Add in new exosome research that reframes “viral” hepatitis as, at least in part, a toxic-stress signaling process, and the case for a one-size-fits-all Day-One dose looks less like public health and more like policy inertia.
Tonight—before the vote—let’s look at what the evidence actually says about risk (near-zero for most infants), efficacy (not the same as antibodies), safety (more complicated than advertised), and biology (exosomes vs. pure germ theory). If ACIP were forced to address these four pillars in open session, tomorrow’s “consensus” might look very different.
When Public Health Propaganda Masquerades as Science
In July 2025, ABC News ran a story titled “RFK Jr., CDC panel have been casting doubt on the hepatitis B vaccine. Here's why it's safe,” painting Robert F. Kennedy Jr.’s skepticism of infant hepatitis B shots as dangerous fringe rhetoric¹. But what’s truly dangerous is the blind endorsement of a policy that gives every newborn a hepatitis B vaccine on Day One of life—despite virtually no epidemiological need in most cases. This is a vaccine program propelled by bureaucratic momentum and pharmaceutical interests, rather than by evidence-based risk–benefit analysis.
Hepatitis B vaccination at birth is touted as a life-saving necessity to thwart a deadly virus. Yet consider the reality: Hepatitis B (HBV) spreads primarily through high-risk adult behaviors—shared needles, unprotected sex, or transmission from an infected mother during birth. These risk factors do not apply to a healthy infant born in a clean hospital to an HBV-negative mother. Such newborns have essentially zero chance of acquiring hepatitis B in infancy². It’s possible for a baby to contract HBV only if the mother is actively infected (something easily screened for), or through an emergency transfusion or rare household exposure. In other words, for the vast majority of newborns, the threat simply isn’t there.
Yet since 1991, the CDC has recommended that every U.S. baby get the HepB shot within hours of birth, no matter how low their risk. There’s no tailoring, no screening—just a blanket mandate. The rationale? Public health officials argue it’s easier to vaccinate everyone than to only target babies at risk. It’s a one-size-fits-all “insurance policy”, allegedly to catch the few cases that might slip through. But this convenience comes at a cost. By treating all infants as if they were IV drug users or sex workers in the making, we expose 100% of them to the potential harms of the vaccine, while offering virtually 0% a tangible benefit at that age¹⁴. In ethical terms, there’s no true informed consent here—parents are seldom told that for an HBV-negative mother’s baby, the chance of contracting hepatitis B is nearly nil, whereas the chance of experiencing the vaccine’s side effects is 100% (every baby’s body must cope with the injection).

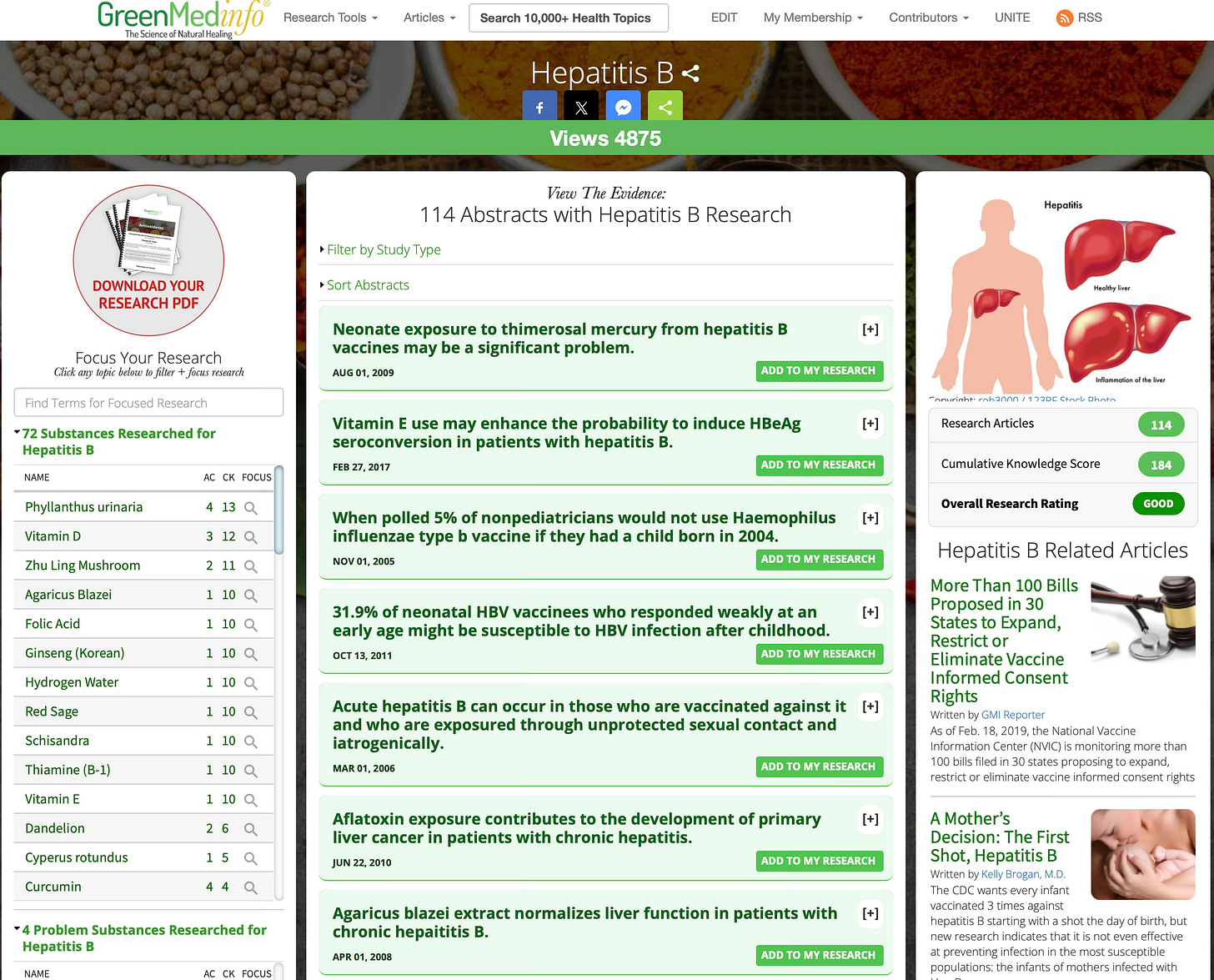
Review 100+ studies on the hepatitis vaccine that challenge the “safe and effective” narrative on the Greenmedinfo.com database.
Even the touted benefits for later in life are dubious. Public health advocates claim infant HepB shots could prevent up to 25 deaths per 100,000 people by averting future infections (a very marginal benefit)¹. But this assumes the vaccine’s protection lasts into adulthood. In reality, it doesn’t. The hepatitis B vaccine’s antibody levels wane over time; by the teenage or adult years when risky behaviors might begin, that infant shot has often worn off³. By the CDC’s own data, any immunity may last at most 15–20 years³. In fact, many children who respond initially will have no measurable hepatitis B antibodies by adolescence. So just when a person might actually need protection, it’s gone. (And that’s assuming the vaccine “takes” at all—about 5–15% of people never mount a sufficient antibody response in the first place, even after all doses.) Moreover, the antibody-based theory of vaccine-induced immunity has undergone profound challenges over the past decade, indicating that serological markers for efficacy such as antibodies alone are insufficient to account for the extremely complex nature of both immunity, infectious disease, and other known and unknown causes of disease, many of which have to do with toxic exposures and nutritional deficiencies and/or intolerances. In short, an infant-shot won’t safeguard someone at 25. It simply front-loads all the risk with none of the reward.
The Context: What Is Hepatitis B, Really?
Hepatitis B is conventionally described as a viral infection of the liver caused by the hepatitis B virus (HBV). Mainstream medicine holds that HBV is a pathogenic invader transmitted via blood or bodily fluids, leading to acute or chronic liver disease. But a growing number of scientists and doctors are re-examining this narrative. They ask: Are viral particles alone truly the lone cause of hepatitis B? Or could the “virus” sometimes be a marker of something else wreaking havoc on the liver?
It’s well-documented that toxic exposures can cause hepatitis (which simply means liver inflammation) without any virus at all. Alcohol abuse, for example, can cause hepatitis. So can certain pharmaceuticals, chemicals, or poisons. Some researchers argue that environmental and toxic factors – such as drugs, pollutants, or even an overstimulated immune response – might trigger the same liver injury that we blame on HBV¹⁵. According to this view, the virus might be more of a signal or accompaniment to liver distress, rather than the root cause in every case. Intriguingly, emerging science on exosomes – tiny communication vesicles that our cells release – blurs the line between what is “virus” and what is an internally generated particle. Viruses and exosomes are strikingly similar in size and structure, and cells under stress (say, from toxins) often release exosome-like particles carrying genetic material. This raises a provocative possibility: What if some of what we call “HBV virus” in the blood are actually exosomal messages from poisoned or damaged cells, not invaders? In the “poisoned-not-infected” framework, toxicity comes first (e.g. exposure to unsafe levels of drugs or metals causes liver cells to suffer), and the viral particles are more like smoke from the fire – the result of cellular injury and inter-cellular communication – rather than the match that lit it.
To be clear, this article does not dispute that HBV exists as a virus, nor that it can be transmitted via blood or sex and cause infection (although this is a topic that could rightfully be discussed in future articles). Here, the contention is that HBV alone may not explain everything about hepatitis B disease. The severity of illness might depend on co-factors – diet, toxins, immune status – and in some cases, those factors might trigger hepatitis even without any virus. This perspective is not yet mainstream, but it’s gaining traction as part of a broader rethinking of “germ theory” in chronic disease. It invites us to consider hepatitis B not purely as an external attack, but as a condition that can also arise from within, when the liver’s cellular environment is poisoned or stressed. In this light, blasting every newborn with a vaccine against the virus could be seen as misdirected – like installing a high-tech alarm system for intruders when the real threat is a gas leak inside the house.
The Mainstream Myth vs. Measurable Reality
Public health authorities promote the hepatitis B vaccine as an unequivocal success story – “safe and effective,” we’re told, with decades of use. In the media, any challenge to this narrative is often met with derision. The ABC News piece, for example, reassured readers that “there’s no evidence that the hepatitis B vaccine leads to autism.” It provided no data or citations for that claim – expecting us to accept it as gospel truth. This is a classic case of eminence-based medicine (appeal to authority) trumping evidence-based medicine. The uncomfortable reality, however, is that hepatitis B vaccination has a long trail of disturbing data behind it, much of which the public has never been made aware of.
Let’s break down the myth versus reality:
Myth: “Newborn hepatitis B vaccination saves lives and has virtually no downsides.”
Reality: For an infant not at risk, the absolute lifesaving potential of the vaccine is essentially zero (since they weren’t going to get the disease to begin with), while the potential downsides – though rare on an individual level – range from short-term reactions to serious long-term injuries.
How serious? The GreenMedInfo research database on hepatitis B vaccination has compiled over 100 peer-reviewed studies documenting a litany of adverse effects⁴. We’ll summarize just a few of the most salient findings here:
Autoimmune Disorders: Multiple studies indicate that the HepB vaccine can precipitate autoimmune problems in susceptible individuals. These include new-onset lupus, rheumatoid arthritis, vasculitis, and others⁵. In one extensive review of vaccine safety data, researchers found compelling evidence – including case reports, case series, and positive re-challenge tests – linking hepatitis B immunization to serious autoimmune diseases. Their conclusion was stark: “One would have to consider that there is a causal relationship between HBV vaccine and serious autoimmune disorders among certain susceptible recipients.”⁵ In other words, for some people the vaccine triggered their immune system to attack their own body.
Neurodevelopmental Delays: Hepatitis B shots (especially those that contained the mercury-based preservative thimerosal in the 1990s) have been examined for links to developmental issues. A notable 2010 study in Journal of Toxicology and Environmental Health found that boys vaccinated as neonates had a threefold higher odds of an autism diagnosis compared to boys who either weren’t vaccinated or were vaccinated later in infancy⁶. This correlation, drawn from a large national survey, doesn’t prove causation, but it raised red flags about vaccinating the developing newborn brain. Critics often dismiss any autism-vaccine connection, but here was peer-reviewed data suggesting a significant association. At the very least, it begged for more investigation – yet health authorities largely ignored it. (It’s worth noting that the HepB vaccine given on Day One delivers a dose of aluminum adjuvant and, historically, sometimes mercury – both neurotoxic metals – into a not-yet-fully-formed blood-brain barrier. The theoretical risk to neurodevelopment is not implausible, which makes the cavalier denial of any link all the more troubling.)
Guillain–Barré Syndrome (GBS): GBS is a rare but serious autoimmune paralysis condition in which the immune system attacks the peripheral nerves. There have been multiple case reports of GBS occurring shortly after hepatitis B vaccination⁷. For instance, a 17-year-old girl in Thailand developed GBS within 3 days of a HepB shot; work-up found no other cause, leading doctors to conclude the “temporal relationship…was suggestive of a vaccine-induced cause.”⁷ While such cases are uncommon, they illustrate how the vaccine can, in very select instances, provoke severe autoimmunity. Even the U.S. Institute of Medicine has acknowledged a biologically plausible link between HepB vaccination and GBS (though data have been deemed insufficient to prove a definitive causal rate).
Anaphylaxis & SIDS: Immediate severe allergic reactions to the hepatitis B vaccine (anaphylaxis) are known to occur in approximately 1 in 600,000 recipients. More controversially, some researchers have reported clusters of sudden infant death syndrome (SIDS) following infant vaccinations, including HepB. For example, a 1992 analysis by pediatrician William Torch found that two-thirds of SIDS cases he reviewed had occurred within 3 weeks of DTP shots. As for HepB, a 1990 paper documented instances of infants who suddenly stopped breathing hours to days after the vaccine⁸. While regulators insist the vaccine isn’t a SIDS trigger, the subject remains under-researched. At minimum, these reports underscore that vaccination can occasionally produce life-threatening reactions – even if rare – in infants who were otherwise stable. Every new parent is typically warned about the risk of SIDS; ironically, they are not warned that one potential risk factor might be the very first injection their baby receives.
Multiple Sclerosis (MS) and Demyelinating Disease: In the mid-1990s, France actually suspended routine HepB vaccination for teens due to a spike in multiple sclerosis cases that were temporally associated with the vaccine. Dozens of studies since have examined whether HepB shots can prompt demyelinating disorders (like MS) in some people. The data is mixed, but a 2018 meta-analysis in Drug Safety concluded that there is evidence of a link in genetically susceptible individuals⁹. In plain terms, the vaccine may act as a trigger for MS or similar neurologic illness in a small subset of people predisposed to autoimmunity. These findings remain contentious (other studies have found no significant association), but the possibility cannot be ruled out. At the very least, patients should be informed and on the lookout for neurological symptoms after vaccination, rather than told “it’s all in your head.”
Hepatic (Liver) Injury: Astonishingly, a vaccine designed to protect the liver might be harming it. Scientists have shown that hepatitis B shots can cause direct liver cell damage in both animal and human studies. A 2012 study in the journal Apoptosis demonstrated that when mouse liver cells (and even mouse muscle cells) were exposed to small doses of the aluminum-adjuvanted HepB vaccine, the cells underwent mitochondrial damage and programmed cell death (apoptosis)¹⁰. The researchers also confirmed signs of liver cell death in mice in vivo after vaccination¹⁰. “Loss of mitochondrial integrity, apoptosis induction, and cell death,” they concluded, all triggered by the vaccine’s components (particularly the aluminum). Another study found that within one day of HepB vaccination, the expression of 144 genes associated with liver metabolism and inflammation was altered in mice⁴. And epidemiological data from the 1990s suggested that children under 6 who received HepB shots had 2.57 times higher odds of liver problems than those who did not⁴. It’s grimly ironic: we may be causing liver dysfunction in children in the name of preventing a liver infection that most of those children would never have gotten.
Systemic Inflammation in Newborns: Italian doctors investigating why some newborns had high inflammatory markers without any infection made a striking discovery. They measured C-reactive protein (CRP) – an inflammation marker – in healthy term infants before and after routine HepB vaccination at birth. After 24 hours, CRP levels spiked significantly in the vaccinated babies (many above levels that would normally indicate sepsis), even though the infants were not sick¹¹. Within a couple days the CRP fell back down, but the message was clear: the vaccine was provoking a strong inflammatory response in these newborns. The authors noted this was the first study to assess CRP after HBV shots in newborns, and that the response could confuse doctors looking for infections. The broader implication is that even when outwardly everything seems fine, an infant’s body may be mounting a major inflammatory reaction to the vaccine – a possible precursor to problems that could emerge down the line (especially with repeated vaccines so early in life).
Chronic Fatigue, Fibromyalgia, and the ASIA Phenomenon: Clusters of cases have linked hepatitis B immunization to the development of chronic fatigue syndrome (CFS) and fibromyalgia-like illness, particularly in young women. Immunologists have a name for this type of problem: “Autoimmune/Inflammatory Syndrome Induced by Adjuvants” (ASIA) – a concept pioneered by Dr. Yehuda Shoenfeld. Essentially, the aluminum adjuvant (and possibly other ingredients) can, in rare cases, kick the immune system into an overzealous, self-attacking mode that leads to chronic disorders. A 2014 study examined 19 patients who developed chronic fatigue and muscle pain following HepB shots. Most were female; many had no prior health issues. On average their symptoms began within about 6 weeks of the vaccination. Over 40% even continued with further doses despite adverse reactions, which unfortunately made some of them worse¹². Almost all of these patients met the criteria for ASIA syndrome, meaning their conditions were very likely vaccine-triggered. While such outcomes aren’t common, they underscore that “long-haul” illnesses can be vaccine injuries too – not just immediate allergic reactions. Fatigue, cognitive issues, widespread pain – these can upend someone’s life every bit as much as a traditional infectious disease might.
Bell’s Palsy (Facial Paralysis): One of the more startling single-case reports involved a young child who developed Bell’s palsy – paralysis of the facial nerve – shortly after a hepatitis B shot. In the 2009 report, doctors detailed how the child’s one-sided facial droop was likely linked to the vaccine, after other causes were ruled out¹³. The paralysis did eventually resolve, but this case and a few others in the literature make it clear that “minor” cranial nerve complications, while very rare, can happen following immunization. When parents notice their baby’s smile has become lopsided post-vaccine, they deserve to know it’s not a coincidence to be casually dismissed; it’s a documented reaction.
Occult Hepatitis B Infections Despite Vaccination: Perhaps the most paradoxical outcome of all is that some vaccinated individuals can still get infected – and not even know it. In babies born to infected mothers, the standard protocol is vaccination plus hepatitis B immunoglobulin (HBIG) at birth. This approach is supposed to be 95% effective at preventing transmission. But a 2013 Journal of Viral Hepatitis study shattered that illusion: using sensitive DNA tests, researchers found that 42% of infants born to HepB-positive mothers still showed signs of “occult” hepatitis B infection by age 2, despite being vaccinated at birth (and many getting HBIG)¹⁴. The vaccine prevented visible, full-blown infection in most cases – these babies didn’t have symptoms or positive standard blood tests – yet the virus still quietly took hold in nearly half of them. “The current practice…is not effective in preventing occult HBV infection in babies,” the authors concluded¹⁴. What’s happening here? It appears the vaccine often pushes the virus into hiding rather than eliminating it. The infant’s immune system, trained only to recognize certain parts of HBV, misses mutant strains or low-level reservoirs that slip past the radar. These “occult” infections can later flare or contribute to liver issues years down the line. In short, even when we follow public health directives to the letter, the promised outcomes (complete immunity and eradication of the virus) don’t always materialize. The complexity of biology outwits our simplistic germ-targeting strategy.
This list could go on, but the point is made: The hepatitis B vaccine – especially as indiscriminately applied in newborns – is far from the perfectly safe, universally necessary intervention it’s portrayed to be. It carries real risks, albeit affecting a minority of recipients, and its long-term benefits are questionable when given so early. If HepB immunization were a new drug being evaluated solely for infants with no exposure risk, it likely wouldn’t pass a truly rigorous risk–benefit test.
Rethinking Infection: Exosomes, Adjuvants, and the “Poisoned-Not-Infected” Paradigm
The evidence of unexpected vaccine injuries and failures compels us to dig deeper into fundamental assumptions. We must ask: Have we gotten the basic biology wrong? The classical Germ Theory of disease – originating from Pasteur – says that microscopic organisms (viruses, bacteria) invade us and cause illness, and thus conquering those germs (with vaccines, antibiotics, etc.) will prevent disease. This theory has indeed explained a lot, but it’s not the whole story of health. Terrain Theory, championed by Bechamp and others, offers a counterpoint: it’s the internal condition of the body (the “terrain”) that determines whether germs cause harm or whether disease develops. In truth, both perspectives have merit, and hepatitis B is a great case study where the simple germ-centric narrative falls short.
Consider again the phenomenon of occult infection despite vaccination. It suggests that the virus was never fully vanquished; it adapted and lingered quietly. The vaccine-focused approach addressed one aspect of the germ, but not the context – the host environment and viral variants. Similarly, when the HepB shot causes liver cell death or autoimmune reactions, it’s a sign that our intervention (aimed narrowly at a virus) triggered a cascade of unintended biological consequences. We introduced a potent mix of antigens and adjuvants (like aluminum) into a vulnerable system and perturbed the terrain. The “exosome biology” viewpoint helps explain how such perturbation can cause what we interpret as pathology: cells under siege (say, from toxic adjuvants or overstimulation) release stress signals (exosomes) that can be mistaken for viruses or can themselves carry harmful signals to other cells. In essence, the boundary between a virus and an exosome is thin – one can turn into the other. A toxin-damaged cell can shed particles that spread inflammatory messages (like a viral infection would). From this angle, injecting an aluminum-adjuvanted vaccine in a newborn could ironically simulate some aspects of an infection – the baby’s body might respond as if something “viral” is happening (hence the CRP spike and interferon responses). In the exosome model, what we call “vaccine reactions” might actually be the body’s attempt to communicate and resolve the cellular stress we just artificially caused.
The “poisoned-not-infected” framework posits that many so-called viral illnesses might actually originate from toxic exposures or other insults, with viruses acting as opportunistic secondary players or messengers. Applying this to hepatitis B: could it be that certain cases of hepatitis (liver inflammation) attributed to HBV were actually due to, say, drug toxicity or malnutrition, with HBV showing up as a bystander? It’s plausible. We know, for instance, that many alcoholics have HBV in their blood (because one risk behavior correlates with another), but their liver damage might be 90% alcohol-induced rather than viral. If we overly credit the virus as the sole villain, we might ignore the “poison” that set the stage. And in terms of prevention, if toxins are the true root cause in many cases, a vaccine won’t stop the damage – but removing or mitigating the toxins would.
Aluminum adjuvant toxicity is a concrete example of the poisoned paradigm. Aluminum salts are included in vaccines like HepB specifically to hyper-stimulate the immune system (so it notices the viral antigen). We now know aluminum can linger in the body, traveling to places like the brain or liver. Researchers like Dr. Chris Exley have raised alarms about aluminum’s role in autoimmune and neurological disorders. A 2011 journal article aptly titled “Mechanisms of aluminum adjuvant toxicity and autoimmunity” outlined how aluminum can disrupt cellular function, kill neurons, and incite chronic immune activation. The HepB vaccine’s pathology aligns with this: the apoptotic liver cell findings, the rise in inflammatory markers, the fatigue syndromes – all are consistent with an immune system revved up and misdirected by a toxic trigger. It’s as if in trying to create an artificial immune response to a virus (that isn’t even there), we’ve accidentally created the same damage that a wild virus (or other poison) would have caused. The “cure” is imitating the disease.
This calls for a paradigm change. Instead of automatically reaching for a pharmaceutical fix for every potential germ, we should evaluate what’s actually harming people and how the body naturally protects itself. Does raising an antibody titer equal immunity? Not necessarily – research in immunology has shown that organisms can clear viruses even without antibodies (through innate immunity and T-cells)¹⁶. Conversely, one can have plenty of antibodies and still fall ill if the overall immune system is compromised or the pathogen evades detection. The fixation on antibodies (the metric by which vaccines are licensed) may be misleading us about true protection. A broader view of immunity – one that includes physical barriers, cellular responses, and yes, exosome-mediated communication – is needed.

Broader Implications: From Germ Warfare to Holistic Health
The story of hepatitis B vaccination is a microcosm of a larger struggle in medicine between two mindsets: one sees health as a battle against external enemies (germs), and the other sees health as the cultivation of a resilient internal environment (terrain). The more we learn, the clearer it becomes that the second view – grounded in biology and systems thinking – must temper the first.
What would a paradigm shift mean in practical terms? It doesn’t mean we abandon all vaccines or all germ theory overnight. But it does mean we start applying some common sense and precision:
Risk-Based Vaccination: Instead of giving HepB shots to every infant “just because,” we must look at the actual risk associated with infection versus the adverse effects of vaccinating a newborn infant. The U.S. took the shotgun route for convenience and higher coverage rates, but we’ve seen the fallout. A risk-based strategy respects individual biology and would spare low-risk infants from unnecessary exposure.
Focus on Maternal Health: Even the conventional medical authorities acknowledge the biggest hepatitis B threat to a baby is an infected mother. Thus, a rational policy would put resources into screening all pregnant women (which we already do) and ensuring infected mothers get treated or managed to reduce transmission. Interestingly, some research indicates that antiviral treatment of high-viremia moms in late pregnancy can further cut down infant infection beyond vaccine/HBIG. But beyond just drugs, if we think terrain-wise: improving the overall health, nutrition, and immune status of the mother can only help the baby. A mother’s liver health, her micronutrient status, absence of toxic exposures – these factors influence whether HBV will pass to baby or how severe it might be. There are also natural, safe, affordable and potentially highly effective interventions that you can find researched on the GreenMedInfo.com database for Hepatitis B
Detox and Strengthen the Terrain: If toxins and poor nutrition can simulate “viral” hepatitis, then removing those factors should be a priority. Public health could emphasize reducing alcohol abuse, addressing the opioid crisis (dirty needle sharing spreads HBV far more than an unvaccinated toddler ever will), mitigating chemical exposures, and strengthening people’s livers (think: less acetaminophen overuse, more antioxidant-rich diets, etc.). By creating a healthier terrain, even those who encounter HBV might have milder illness or clear it without chronic damage. In fact, acetaminophen (i.e. Tylenol) toxicity can itself mimic viral infection. Reach the article below to learn more about this astounding fact.
Reframing Viral Mechanisms: Exosomes, Toxicity, and the Xenogen Hypothesis
·
In a 2018 study published in Scientific Reports, researchers explored the effects of acetaminophen-induced liver injury in mice, with an initial focus on validating toxicological mechanisms of liver damage. However, their findings inadvertently cast light on a much deeper—and potentially paradigm-shifting—insight into the nature of so-called "viral" dis…
Transparent Vaccine Safety Science: We need to squarely acknowledge vaccine injuries and the manipulation or cover up of research on vaccine safety issues (or reconsider uses where risk outweighs benefit). The current system largely denies or downplays reports like those we’ve discussed. Doctors are taught that “it’s just a coincidence” if a baby’s issues start after a shot. This breeds distrust. Imagine instead a system that openly says, “Yes, hepatitis B vaccination has been linked in rare cases to autoimmunity, neurological issues, and more. Here’s what we estimate the rates to be, here’s who might be at higher risk (e.g., families with autoimmune disorders), and here’s what warning signs to watch for after injection.” Such honesty would allow parents and providers to make informed decisions. Maybe some would still choose the newborn shot, many likely would not – but in any case, informed consent would be respected, not steamrolled.
Reevaluating Aluminum Adjuvants: Given the evidence of harm, it’s time to demand alternatives to aluminum in vaccines (or prove it safe at current doses, which has never been conclusively done) - and alternatives to the vaccines themselves. The fact that a standard U.S. baby could receive nearly 1,000 micrograms of aluminum across multiple shots at a single visit is biologically concerning. Regulators have assumed it’s fine, but science indicates otherwise. If exosome biology tells us anything, it’s that when cells are stressed by such adjuvants, they will respond, for better or worse. Let’s not ignorantly provoke that response.
Integrating Exosome Research in Virology: The exosome perspective opens exciting avenues for therapy. If some viruses are riding on exosomes or indistinguishable from them, could we develop strategies to modulate exosome production or uptake to treat viral diseases? For instance, some researchers are looking at exosome-based diagnostics and even using exosomes as drug delivery systems. The blurred line between self and “other” that exosomes represent might help explain phenomena like autoimmunity (the body reacting to its own exosomal messages) and persistent viral infections. By incorporating this knowledge, medicine can move beyond the blunt instrument of “just stimulate antibodies” and toward more nuanced and natural interventions that truly support the body’s healing processes.
Conclusion: Toward a New Paradigm of Health – Biology over Ideology
Rethinking hepatitis B vaccination is not just about one vaccine or one disease. It’s about how we approach human health at the most fundamental level. Do we trust a $30 shot more than the intricate immune system shaped by millions of years of evolution? Do we value biological integrity or bow to ideological rigidity? The current paradigm has been heavy on the latter – an almost religious adherence to “vaccination über alles,” where raising any concern is heresy. This has to change.
A new paradigm grounded in biology would prioritize listening to the body’s signals. When so many independent studies report vaccine-related harms, that is the body (collectively, of many individuals) telling us something is wrong. It’s not an attack on science to heed those signals – it is science. Likewise, when evidence mounts that a germ-focused intervention isn’t delivering as promised (e.g., infants still getting occult HBV infections; adult cases of hepatitis B arising in fully vaccinated people), it’s a sign that our strategies must evolve. Health should not be a zero-sum “war on microbes” but rather a collaborative effort to optimize the human ecosystem. Sometimes that means using vaccines or antibiotics – but much of the time it means bolstering nutrition, ensuring clean water and air, reducing toxic load, and tailoring healthcare to individual needs.
Perhaps nowhere is reform more needed than in the newborn nursery, which has become a conveyor belt for injections and procedures that parents barely understand. The decision to vaccinate a baby on Day One of life with a biologic aimed at an adult disease is, when you step back, quite extraordinary. As our work at GreenMedInfo has pointed out over almost two decades, “the first shot is the deepest” – it sets the tone for a lifetime of medical interventions or lack thereof. Parents deserve the right to weigh that decision with full transparency. After all, they are entrusted with that child’s well-being for life; a hospital or public health official is not.
In challenging the status quo on hepatitis B, a larger truth comes into focus: public health should serve the public, not the other way around. The tools of public health which far too long has relied on an ever-expanding vaccine schedule, with a one-size-fits-all model that is not scientifically ground, nor backed by proper vaccine safety studies, must evolve to find safer, more effective, and natural approaches. If those tools aren’t actually benefiting a particular group (here, newborns) or are even harming them, then dogmatic insistence on their use is indefensible. A health system grounded in biology would adjust course in light of new evidence; a system grounded in ideology doubles down and covers up. It’s time to choose the former.
In the end, the shift we seek is a shift from fear to trust: fear in microbes and mandates, to trust in biology and informed choice. It’s a long road, but every step – including rethinking something as ingrained as newborn HepB shots – is progress. The health of the next generation depends on our willingness to travel this road, however uncomfortable it may be for the institutions that got us here. Truth and transparency must light our way. Only then can we truly claim to practice evidence-based medicine, rather than medicine based on inertia and authority. The hepatitis B debate is an inflection point; from it, let a new paradigm be born.
To learn more about this new paradigm, I encourage you to watch my recent presentation on the topic below.
Genes, Germs, and the Myth of the Invisible Enemy: Toward a New Model of Health

"For over a century, the narratives of germ theory and genetic determinism have shaped the dominant view of health, casting invisible enemies—germs and faulty genes—as the primary causes of disease. This model, while persuasive, has fostered a culture of fear, disempowerment, and dependency, divorcing individuals from the deeper realities of health and …
References:
ABC News – “RFK Jr. Questions CDC Panel Casting Doubt on Hepatitis Vaccine.” (2025). (Mainstream media piece framing HepB vaccine skepticism as dangerous).
Stevenson, H. “Hepatitis B: Risk to Newborns of Uninfected Mothers.” (GreenMedInfo, 2012) – Notes that HBV is spread by sex/blood and mothers can be screened, thus “no plausible risk to newborns of non-infected mothers.”
Stevenson, H. Ibid. – Points out CDC’s own data show HepB vaccine immunity may last at most ~20 years, meaning “just when a child is entering the age of greatest sexual activity, the vaccination provides no benefit.”Also questions efficacy even when fresh.
Stevenson, H. “HepB Vaccine Causes Liver Disease – Science Shows How.” (GreenMedInfo, 2012) – Summarizes research that HepB vaccine with aluminum causes liver damage. Reports in vivo mouse study: 144 liver genes altered post-vaccine; a 1990s analysis found children <6 who got HepB shots were 2.57× more likely to have liver problems.
Geier, M. & Geier, D. “Hepatitis B Vaccination and Autoimmune Disorders.” Clin. Exp. Rheumatol.22(6):749-55 (2004). – Review of VAERS and case reports. Found numerous cases of lupus, arthritis, Guillain–Barré, MS, etc., after HepB vaccination. Notably, 465 instances of symptoms returning/worsening upon re-challenge. Concludes a “causal relationship between HBV vaccine and serious autoimmune disorders” is likely in susceptible individualspubmed.ncbi.nlm.nih.govpubmed.ncbi.nlm.nih.gov.
Gallagher, C. & Goodman, M. “Hepatitis B Vaccination of Male Neonates and Autism Diagnosis.” J. Toxicol. Environ. Health A 73(24):1665-77 (2010). – Cross-sectional study of U.S. children. Boys who got HepB vaccine in the first month of life had 3× higher odds of autism compared to those unvaccinated as neonates. “Boys vaccinated as neonates had threefold greater odds for autism diagnosis…” the authors reportpubmed.ncbi.nlm.nih.govpubmed.ncbi.nlm.nih.gov.
Sinsawaiwong, S. et al. “Guillain–Barré Syndrome Following Recombinant Hepatitis B Vaccine: A Case Report.” J. Med. Assoc. Thai 83(9):1124-6 (2000). – A 17-year-old developed GBS within 3 days of HepB shot. Work-up excluded other causes. “The temporal relationship…was suggestive of a vaccine-induced cause,”authors statepubmed.ncbi.nlm.nih.gov. (Additional: Souayah et al., 2009, analyzed VAERS: found GBS occurred after various vaccines including HepB, but data were inconclusive on excess risk.)
Bertuccio, C. et al. “Adverse Events and Sudden Death after Hepatitis B Immunization in Infancy.” Adv. Exp. Med. Biol. 272:183-95 (1990). – Collected reports of infants who experienced apnea, anaphylaxis, or sudden death shortly after HepB vaccination. While rare, these events were documented in medical literature, highlighting that severe acute reactions (including SIDS) can temporally follow vaccination.
Mouchet, J. et al. “Hepatitis B Vaccination and Central Demyelinating Diseases: A Review.” Drug Safety41(8):767-77 (2018). – Examined multiple studies on HepB vaccine and MS risk. Concluded that evidence is mixed, but certain studies indicate a possible link between HepB immunization and demyelinating diseases (like MS), particularly in individuals with genetic susceptibility. (E.g., a 2017 analysis by Bouillon et al. found increased MS risk in a specific subgroup of vaccinated adults.)
Hamza, H. et al. “Hepatitis B Vaccine Induces Apoptotic Death in Hepa1–6 Cells.” Apoptosis 17(5):516-27 (2012). – Laboratory study demonstrating HepB vaccine (with aluminum) causes programmed cell death in mouse liver cells and muscle cells at low doses. Also observed apoptosis in mouse liver tissue in vivo after vaccination. Concludes: “exposure of Hepa1–6 cells to a low dose of adjuvanted hepatitis B vaccine leads to loss of mitochondrial integrity, apoptosis induction, and cell death… In vivo apoptotic effect…was observed in mouse liver.”pubmed.ncbi.nlm.nih.gov. (This directly shows the vaccine can harm liver cells.)
Celik, I.H. et al. “Inflammatory Responses to Hepatitis B Vaccine in Healthy Term Infants.” Eur. J. Pediatr.172(6):839-42 (2013). – Clinical trial measuring C-reactive protein (CRP) and IL-6 in 70 newborns before/after HepB vax. CRP was significantly elevated 24h post-vaccine in many infants (22 of them had CRP above levels suggestive of infection, despite being clinically well). Authors warn that HepB vaccine “is responsible for CRP elevation in term infants after vaccination at birth” and that this should be accounted for to avoid confusion with neonatal sepsis¹¹pubmed.ncbi.nlm.nih.govpubmed.ncbi.nlm.nih.gov.
Agmon-Levin, N. et al. “Chronic Fatigue Syndrome and Fibromyalgia Following HBV Vaccination: Another Aspect of ASIA.” Immunol. Res. 60(2-3):376-83 (2014). – Case series of 19 patients who developed chronic fatigue and/or fibromyalgia after hepatitis B shots. Most were young adult females; ~21% had personal/family autoimmunity history. Symptom onset ranged from days to up to 1 year post-vaccine (mean ~39 days). Common issues: neurological problems (84%), musculoskeletal pain (79%), cognitive/psych disturbances (63%), profound fatigue (63%). All patients met the criteria for autoimmune/inflammatory syndrome induced by adjuvants (ASIA), implicating the vaccine’s aluminum adjuvant as a trigger¹² pubmed.ncbi.nlm.nih.govpubmed.ncbi.nlm.nih.gov.
Alp, H. et al. “Bell’s Palsy as a Possible Complication of Hepatitis B Vaccination in a Child.” J. Health Popul. Nutr. 27(5):707-8 (2009). – Case report of a child who developed Bell’s palsy (facial nerve paralysis)shortly after a HepB dose. Work-up found no infections or causes besides recent immunization. Authors consider the vaccine the likely trigger, though such an adverse effect is very rare. (This case is cited as an example of unexpected neurological reactions in pediatric vaccination) pubmed.ncbi.nlm.nih.gov.
Pamphilon, D.H. et al. (study authors); cited in Ji, S. “FAIL: Infant Hep B Vaccines Perform Shamefully; Time to End Them?” (GreenMedInfo, 2013) – Reports on a randomized trial (J. Viral Hepat. 2013) where 42% of babies born to HBsAg-positive mothers showed “occult” HBV infection by 2 years old despite full vaccination (and HBIG in half the cases). “42% of babies…develop occult HBV infection, which is not prevented by…HBV vaccine,” researchers found¹⁴. Overt disease was reduced, but the virus often went into hiding (escaped immune detection). Challenges claims of 95% efficacy in preventing mother-to-infant transmission.
Trepo, C. & Guillevin, L. “Does Hepatitis B Virus Alone Cause Hepatitis B? Reconsidering the Role of Co-factors.” Med. Hypotheses 70(2):346-8 (2008). – Hypothesizes that toxic and environmental co-factors (like aflatoxin exposure, alcohol, co-infections) significantly influence the development of hepatitis B and its complications. Suggests that in some cases, chemical triggers might initiate liver injury with HBV acting as a secondary factor. (Supports the idea that hepatitis B is not purely a viral cause-and-effect disease).
Jayaratne, J. et al. “Protective Immunity Without Antibodies: Lessons from Immunity to Viral Infections.”Immunity 37(3):412-22 (2012). – Study showing that mice could clear certain viral infections even when they couldn’t produce antibodies, by relying on innate immune mechanisms. Underscores that antibody titers alone are not a perfect proxy for immunity¹⁶. In context, a HepB vaccine can generate high antibody levels yet still fail to prevent infection (if the virus mutates or immunity wanes), whereas a robust innate response might stop hepatitis B without any vaccine at all. This nuance challenges the core vaccinology assumption that “antibody = protection” in all cases.
No hay comentarios:
Publicar un comentario