Sayer Ji
May 28, 2026
Dr. Newport couldn’t watch her husband disappear into Alzheimer’s, so she went looking for a fuel his brain could still burn. What she found in a kitchen pantry — and what 99% of pharmaceutical research has failed to deliver in two decades — is a story about biology, money, and asking the wrong question.
The Clock That Couldn’t Be Drawn
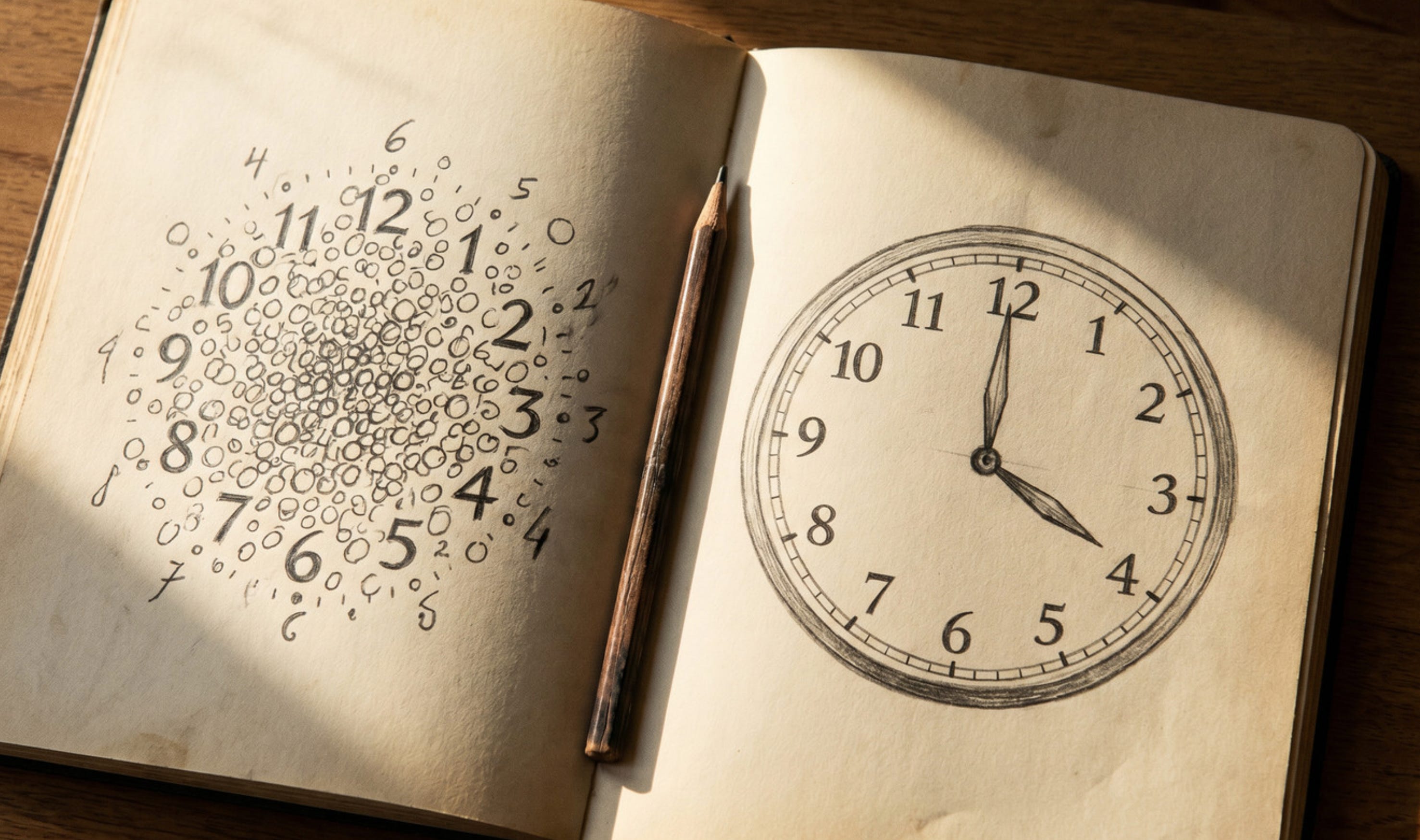
In May 2008, Dr. Newport — a Florida neonatologist — watched her 58-year-old husband Steve try, and fail, to draw a clock. He drew “a few little circles and several numbers just in a very random pattern.” The doctor pulled her aside and told her Steve was “beyond moderate” Alzheimer’s, on the verge of severe (US Against Alzheimer’s). The tremors had started. The reading was gone. The man she had married 40 years earlier was disappearing.
Two days later, after staying up reading patent applications instead of sleeping, she began adding coconut oil to his breakfast. Two weeks later he drew the clock again — recognizably a clock (TEDx: Mary Newport). Within months he was running. He could read. His humor came back (CBN News, 2013).
This is the story of what Newport found in that patent application — and why, eighteen years later, pharma’s $42 billion Alzheimer’s bet is collapsing while a tropical fat in every grocery store keeps outperforming expectation.
The 99% Failure Pharma Doesn’t Like to Talk About
Since 2003, approximately 99% of Alzheimer’s drug trials have failed to live up to expectations (Cummings, Alzheimer’s Research & Therapy, 2019); one analysis pegs the pipeline failure rate at 99.6% (Life Sciences, 2022). For disease-modifying therapies the failure rate has been 100% (Cummings, 2019) approved despite
The drugs that reached market — aducanumab, lecanemab, donanemab — were all built on the amyloid hypothesis: sticky beta-amyloid plaques cause cognitive decline. Aducanumab failed both Phase 3 trials, was resurrected via accelerated FDA approval in 2021 despite the overwhelming opposition from the FDA’s advisory committee regarding the evidence of efficacy, then quietly discontinued. Lecanemab and donanemab clear plaques and slow decline by margins most clinicians call marginal — at a documented cost in brain swelling (ARIA-E) and brain bleeds (ARIA-H). In CLARITY AD, 17.3% of lecanemab patients developed brain bleeds and 12.6% developed brain swelling (van Dyck et al., NEJM, 2023; Eisai trial summary). In the high-dose aducanumab Phase 3 trials, 41% developed ARIA (Salloway et al., JAMA Neurology, 2022).
In TRAILBLAZER-ALZ 2, ARIA-E occurred in approximately 24% of donanemab-treated participants, while ARIA-H occurred in roughly 31%, including several treatment-related deaths. (Sims et al., JAMA, 2023; biochempeg summary).
Worse, the foundational science is under formal investigation. A 2022 Science exposé revealed image manipulation in the 2006 Nature paper that became the most-cited foundation of the amyloid model (Piller, Science, 2022). HHS Secretary Robert F. Kennedy Jr. has described the amyloid pipeline as built on “utter corruption” (Science, May 14, 2025), and in January 2026 he appointed a new Federal Alzheimer’s Advisory Council chair and ten new members tasked with broadening the agenda beyond amyloid. To Senator Susan Collins he committed: “We have an opportunity now to do really good science and find a cure very quickly, and also find out, equally importantly, why so many people are getting Alzheimer’s in this generation” (Collins press release, May 14, 2025).
The pushback was swift, coordinated, and almost entirely from “patient advocacy” organizations whose financial dependencies merit a closer look. The Alzheimer’s Association issued a June 2025 statement explicitly accusing Kennedy of “mischaracterizing” Alzheimer’s research — singling out his invocation of the Type 3 diabetes framing as “inaccurate and misleading,” with CEO Maria Carrillo insisting that “calling insulin dysfunction in the brain ‘diabetes’ obscures and oversimplifies complex diseases and risks misinforming the public.” That is a striking position to take against twenty years of peer-reviewed neurometabolic literature.
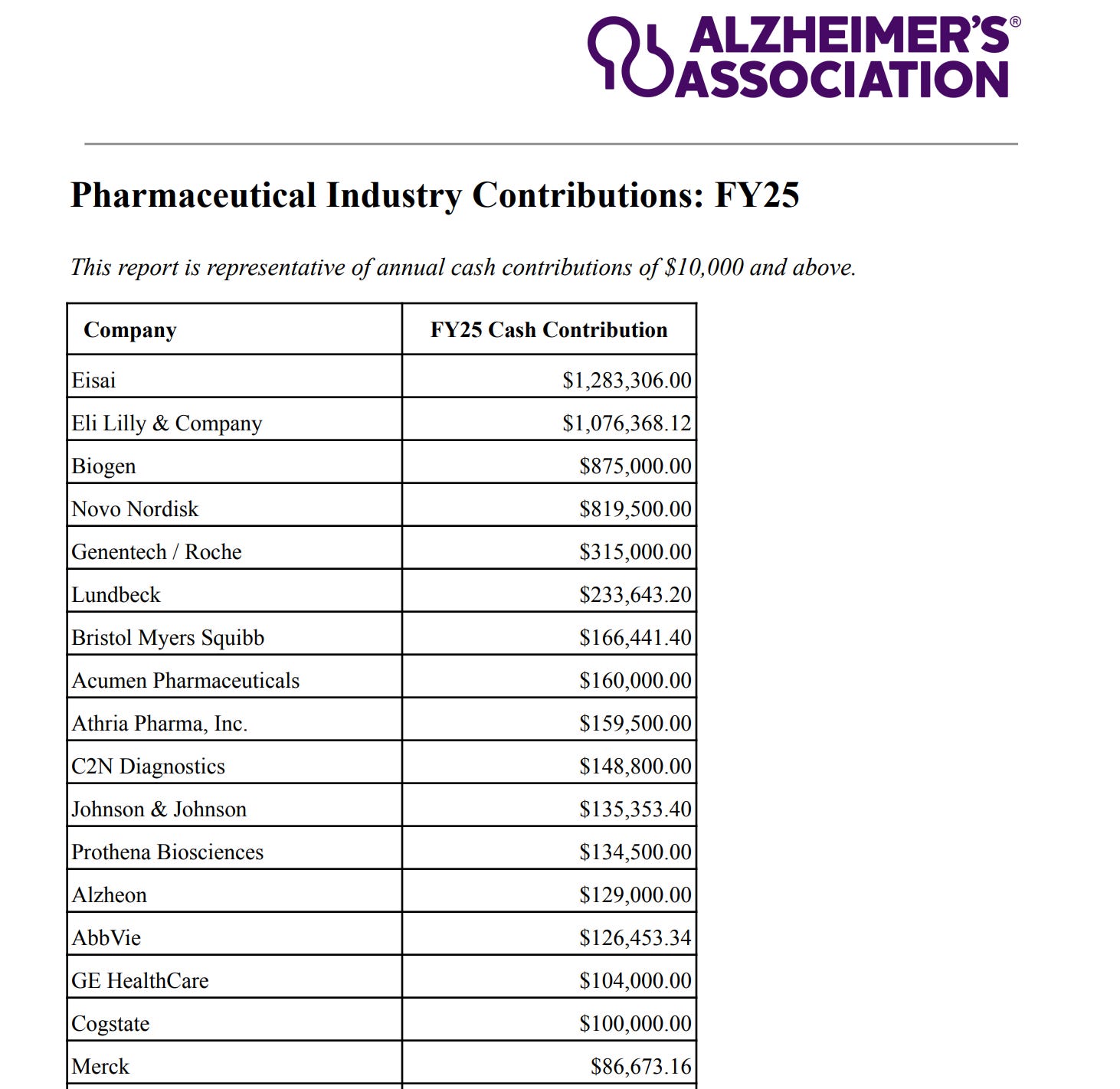
The context the press release omits is who pays the rent. The Alzheimer’s Association’s own FY25 industry contributions disclosure — voluntarily published on its website — shows the organization received $1.28 million from Eisai, $875,000 from Biogen, and $1.08 million from Eli Lilly in a single fiscal year. Eisai and Biogen co-market lecanemab. Biogen developed aducanumab. Eli Lilly developed donanemab. These three companies — the makers of the entire amyloid-antibody franchise Kennedy is now questioning — are the Association’s three largest pharmaceutical donors, contributing over $3.2 million combined. Add Genentech/Roche, AbbVie, Johnson & Johnson, Novartis, Merck, Takeda, and the rest of the disclosed roster and the Alzheimer’s Association looks less like an independent patient-advocacy group and more like the public-relations arm of the amyloid pipeline. Its defense of the orthodoxy is not science. It is a balance sheet.
What Kennedy is pointing at, whether he names it or not, is the same biology Mary Newport found in a patent application in 2008.
Type 3 Diabetes: The Real Story of the Failing Brain
In 2005, Brown University researchers led by Dr. Suzanne de la Monte examined the brains of Alzheimer’s patients with no history of diabetes. They found insulin resistance and insulin deficiency in every brain, and coined the term Type 3 diabetes (de la Monte & Wands, J. Diabetes Sci. Tech., 2008). The dysfunction begins 10 to 20 years before symptoms (de la Monte, 2014).
Glucose entry into a neuron depends on insulin signaling. When signaling fails, the cell starves in a sea of sugar — and decreased cerebral glucose metabolism is one of the earliest Alzheimer’s signs on PET, visible years before symptoms (Cunnane et al., Annals NYAS, 2016).
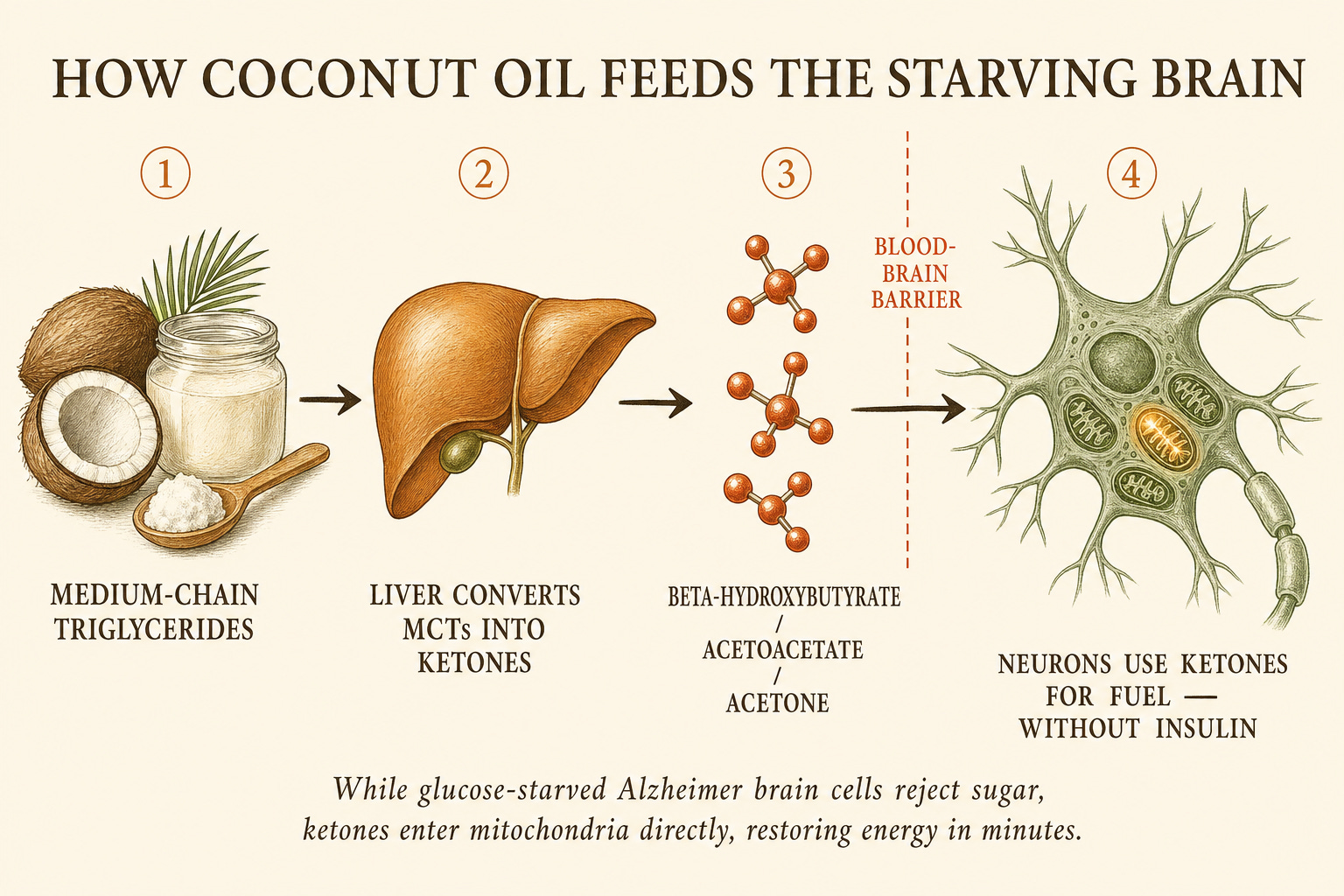
But neurons have a backup fuel. Within ~36 hours of carbohydrate restriction, the liver converts fatty acids into ketone bodies — beta-hydroxybutyrate, acetoacetate, acetone — water-soluble molecules that cross the blood-brain barrier and enter mitochondria without requiring insulin. The starving brain switches fuel and lights back up.
This single insight explains both why the amyloid drugs have failed and why a spoonful of coconut oil produces changes visible within hours.
How Coconut Oil Becomes Brain Fuel
Coconut oil is roughly 66% medium-chain triglycerides (MCTs) by weight — predominantly caprylic acid (C8), capric acid (C10), and lauric acid (C12). Unlike long-chain fats, MCTs bypass bile-salt absorption, travel directly from gut to liver via the portal vein, and are oxidized into ketone bodies within minutes (Cunnane, 2016).
A landmark 2004 NIH-on-Aging study gave 20 adults with Alzheimer’s or MCI a single dose of MCTs. Within 90 minutes, beta-hydroxybutyrate rose significantly — and on cognitive testing, paragraph recall improved in direct proportion to the ketone rise (Reger et al., Neurobiology of Aging, 2004; GreenMedInfo). One dose. Two hours. Measurable improvement.
In 2017, a Journal of Alzheimer’s Disease study exposed live rat cortical neurons to amyloid-beta — the same molecule pharma has spent decades trying to clear — and found that coconut oil rescued the neurons from amyloid-induced mitochondrial damage, preserving normal mitochondrial shape (Nafar et al., reviewed at GreenMedInfo). Not plaque clearance — metabolic rescue.
GreenMedInfo’s coconut oil database now indexes nearly 100 studies across 88 disease states, with neurological benefits the largest category (Stroke entry); the MCT page compiles human trials in epilepsy and dementia. Even coconut water — fat-free, containing the cytokinin trans-zeatin — inhibits amyloid-beta neurotoxicity and acetylcholinesterase in preclinical models (GreenMedInfo).

The University of South Florida’s Byrd Alzheimer’s Institute eventually launched the first randomized crossover trial of coconut oil in mild-to-moderate Alzheimer’s (USAA, March 2015) — a quiet concession that the anecdotal signal could no longer be ignored.
Why You’ve Never Heard of It
Coconut oil sells for fifteen dollars a jar. It is unpatentable. It generates no royalty stream, supports no sales force, funds no CME credits, underwrites no journal supplements. The economic logic of pharmaceutical research is structurally incapable of metabolizing it.
Compare it to lecanemab: $26,500 per patient per year, infusion infrastructure, MRI surveillance for brain bleeds, a clinical effect most geriatricians call marginal. Compare it to the Ketone Ester developed by Prof. Kieran Clarke at Oxford — roughly 10× more potent than coconut oil at raising blood ketones. As Clarke noted in 2013, her lab cannot scale because “there’s no profit in manufacturing stuff like that” (CBN News). The molecule that would most directly deliver Newport’s intervention sits stranded for lack of a business model.
This is what people mean when they say the medical-industrial complex has structural blind spots. It is not a conspiracy. It is a bookkeeping problem with neurological consequences — and exactly the kind of problem any serious NIH reform the new Advisory Council claims to pursue would have to confront to be more than rhetoric.
What To Do, Practically

The protocol Newport developed and that subsequent research has refined:
Begin with 1–2 teaspoons of organic, non-hydrogenated, virgin coconut oil per meal, working up to 4–6 tablespoons daily as tolerated. Avoid hydrogenated coconut oil (trans fats) (CBN News).
Combine with MCT oil (caprylic/capric acid) for faster, higher ketone elevation (Reger, 2004).
Reduce dietary sugar and refined carbohydrate to address the underlying insulin resistance, not just supply backup fuel.
Layer the broader neuroprotective evidence base: turmeric/curcumin, Mediterranean diet, B vitamins, resveratrol, ginkgo — full database here.
None of this is a cure. None replaces clinical care. But it is a metabolic intervention grounded in published biology, available at any grocery store, costing less than a co-pay, with eighteen years of accumulating evidence behind it.
The Question Behind the Question
The deepest lesson of the Newport story isn’t that coconut oil treats Alzheimer’s. It’s that the question pharma asked for thirty years was the wrong question. The amyloid plaque is not the fire. It is the smoke. The fire is metabolic — a slow starvation of neurons cut off from their fuel by insulin signaling that the modern diet, environmental toxic load, and chronic inflammation have systematically corrupted (de la Monte, 2014).
You cannot solve a metabolic disease with a monoclonal antibody. You solve it by restoring the metabolism — feeding the cell what it can still burn, removing what is poisoning the signaling pathways, and treating the brain as the energetically expensive organ it has always been.
Mary Newport found this at three in the morning because her husband was running out of time. The pharmaceutical industry has had every dollar, every researcher, every regulatory advantage, and eighteen years — and what it delivered costs $26,500 a year and bleeds into the brain.
The coconut was in the kitchen the whole time.
Learn more by watching below Dr. Mary Newport’s video below.
Interested in learning more about natural approaches to dementia and Alzheimer’s? Join the GreenMedInfo.com community here and support our free service giving access to over 100,000 studies to the world by doing so.
Share the X thread dedicated to this article on X:

Sayer Ji is the founder of GreenMedInfo.com. The full coconut oil research database — nearly 100 indexed studies across 88 health conditions — is available at greenmedinfo.com/substance/coconut-oil. The companion Alzheimer’s disease research portal is at greenmedinfo.com/disease/alzheimers-disease.
No hay comentarios:
Publicar un comentario