Sayer Ji
May 23, 2026

In May 2026, RFK Jr. fired two vice chairs of the U.S. Preventive Services Task Force (USPSTF) — the body whose letter grades legally determine what preventive care your insurance must cover — and the medical establishment and its media apparatus erupted in performative outrage. The concern was presented to the public in the following terms: that political operatives would replace evidence-based scientists, that mammograms and colonoscopies would go the way of vaccine recommendations. But in the ensuing media storm, almost no one stopped to ask a harder question. What if the evidence base for mammography screening was already contested, complicated, and in some dimensions, quietly devastating — long before any politician arrived to interfere?

I. Detection Is Not Prevention
The War on Cancer’s Category Error
When the USPSTF issues an “A” or “B” grade for mammography, it is grading a screening procedure — the capacity to detect abnormal cells in breast tissue before they produce symptoms. What it is emphatically not grading is any intervention that reduces the biological conditions in which breast cancer arises. This is the foundational category error of modern oncological prevention: it conflates early detection with prevention, and treats the two as equivalent.
They are not equivalent. A mammogram cannot reduce systemic inflammation. It cannot reverse intestinal hyperpermeability — the “leaky gut” phenomenon through which microbial products translocate into systemic circulation and drive the chronic immune dysregulation that provides fertile terrain for cancer proliferation.[1]
It cannot alter the epigenetic expression of tumor-suppressor genes. It cannot change the microRNA profile of a woman’s cells, which determines whether oncogenic pathways are silenced or amplified.[2] What a mammogram can do is find something — and in finding it, set in motion a cascade of interventions whose benefits, when examined rigorously, are far more modest than their cultural mythology suggests.
Estimated number of American women overdiagnosed by mammography screening over a 30-year period — treated for cancers that would never have caused symptoms or death — according to a landmark 2012 analysis in the New England Journal of Medicine.[3]
II. The Overdiagnosis Problem
When Finding Is Not the Same as Saving
Overdiagnosis in breast cancer screening refers to a specific, clinically documented phenomenon: the detection by mammography of a cancer — a real cluster of abnormal cells — that would never, in the lifetime of that woman, have caused symptoms, spread, or killed her. Her body’s immune surveillance was managing it. Her epigenetic terrain was containing it. Once detected, however, it becomes a diagnosis. A breast cancer diagnosis. And the institutional logic of oncology treats that diagnosis with the full arsenal: biopsy, surgery, radiation, and often years of hormone suppression therapy.[4]
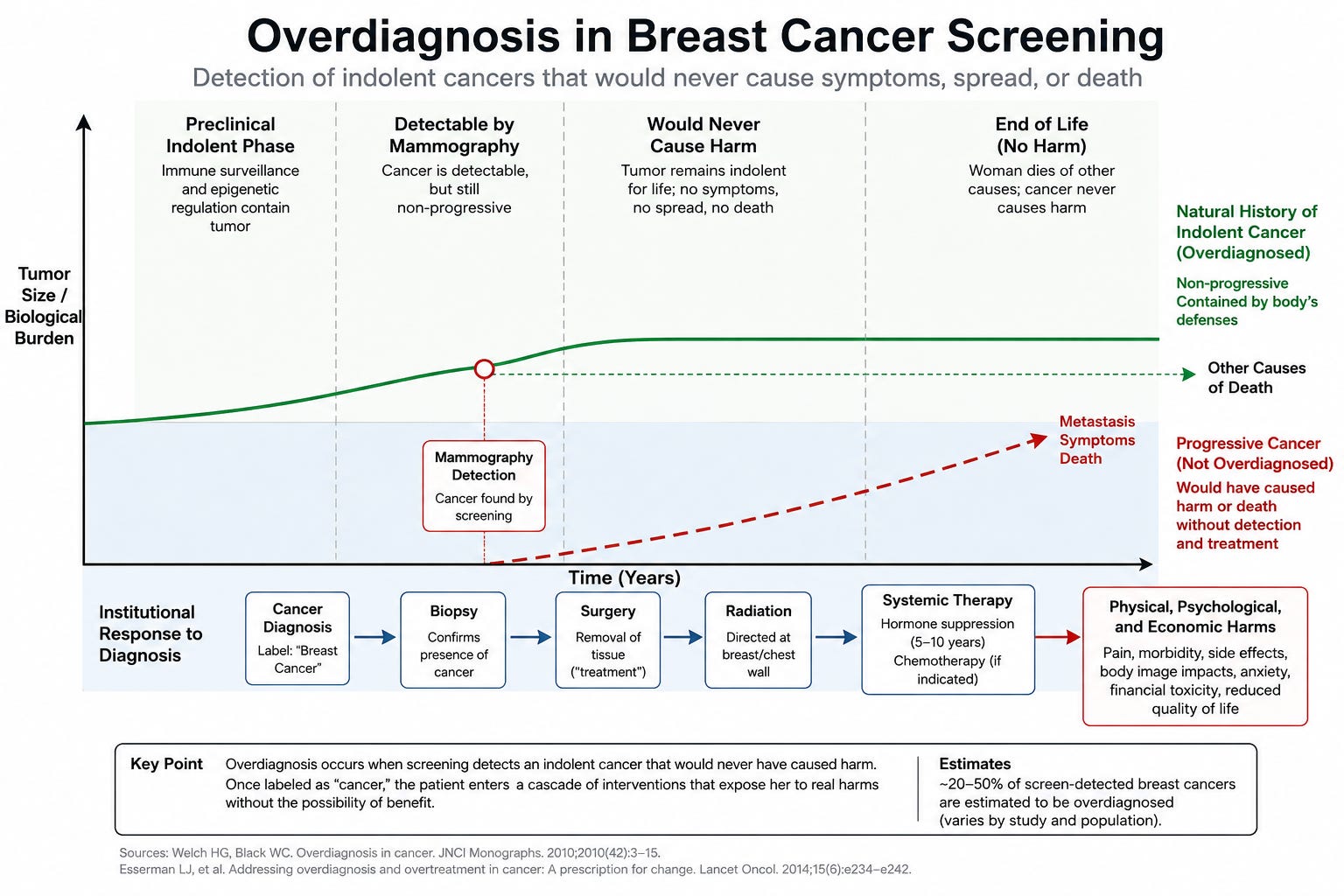
The woman is counted as a “breast cancer survivor.” She credits the mammogram with saving her life. The system counts her as a success. In fact, she may have been harmed — treated for a condition that posed no threat, subjected to interventions whose aggregate toxicities are not trivial — while the conditions that created her abnormal cell population remain completely unaddressed.
Estimates of overdiagnosis magnitude range from 11% to over 50% of screen-detected breast cancers.[5] A 2012 analysis in the New England Journal of Medicine found that in the three decades following the widespread adoption of mammography, the rate of early-stage breast cancer diagnoses doubled, while late-stage cancer decreased by only a small fraction — suggesting that most of the additional diagnoses were overdiagnoses, not cancers caught early enough to prevent metastasis.[3]

III. The DCIS Epidemic
A Diagnosis Created by the Technology That Finds It
The single largest driver of mammographic overdiagnosis is ductal carcinoma in situ — DCIS. Virtually unknown before widespread screening, DCIS is now the fourth most common cancer diagnosis in women in the United States, accounting for roughly 20% of all breast cancer diagnoses.[7] DCIS describes the proliferation of abnormal cells within the milk duct — not invasive cancer. A cellular abnormality. A tissue-level change. A finding.
The standard of care for DCIS has been aggressive: lumpectomy or mastectomy, followed by radiation, followed often by years of tamoxifen. Women have lost breasts for DCIS. And the evidence is now accumulating — from randomized controlled trials, from natural history studies — that the majority of low- and intermediate-grade DCIS lesions do not progress to invasive cancer.[8] The body, in many cases, was containing them.
Learn more by reading my article below:

This author has tracked this evidence since 2008 — and the landmark COMET trial, presented at the San Antonio Breast Cancer Symposium, has now validated what a decade of advocacy argued: active monitoring is equally safe as surgery for most DCIS.
This maps directly onto the framework of epigenetics and genetic penetrance: having a gene variant does not mean the disease will express. Having abnormal cells in a duct does not mean they will invade. The epigenetic terrain — the inflammatory milieu, the microbiome integrity, the dietary information environment, the toxicant burden — determines whether latent dysregulation progresses or resolves. As I wrote in Regenerate: “Genes load the gun, but environment pulls the trigger.”[9]

IV. The BRCA Mythology
Prophylactic Surgery and the Genetics of Fear
No dimension of mammographic overtreatment is more dramatic than the story of prophylactic mastectomy in BRCA-positive women. Following Angelina Jolie’s widely publicized decision in 2013 to have both breasts and her ovaries surgically removed based on BRCA1 status, rates of contralateral prophylactic mastectomy in the United States increased sharply.[10] The procedure — permanent, irreversible, with significant complication profiles — was embraced as rational prevention.
As documented in my 2023 analysis, the USPSTF's own draft modeling report explicitly acknowledged it did not consider "potential risk of breast cancer due to screening-related radiation" — meaning the carcinogenic risk to BRCA-positive women from the screening tool itself was never factored into its recommendations.
The biology, however, does not support the cultural narrative. According to data published in The Lancet Oncology, BRCA-positive women with breast cancer have higher survival rates than BRCA-negative women diagnosed with the same disease.[11] Thousands of polymorphisms in the BRCA1 and BRCA2 genes have been identified — some inversely related to cancer risk, and some, like the BRCA1 subtype K1183R, that actively increase breast cancer survival.[12]

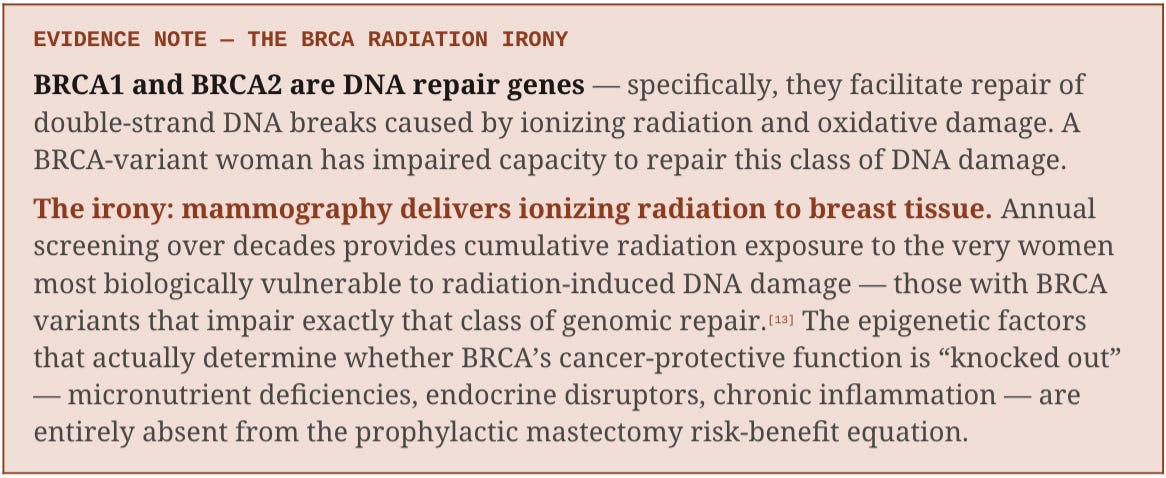
EVIDENCE NOTE — THE BRCA RADIATION IRONY
BRCA1 and BRCA2 are DNA repair genes — specifically, they facilitate repair of double-strand DNA breaks caused by ionizing radiation and oxidative damage. A BRCA-variant woman has impaired capacity to repair this class of DNA damage.
The irony: mammography delivers ionizing radiation to breast tissue. Annual screening over decades provides cumulative radiation exposure to the very women most biologically vulnerable to radiation-induced DNA damage — those with BRCA variants that impair exactly that class of genomic repair.[13] The epigenetic factors that actually determine whether BRCA’s cancer-protective function is “knocked out” — micronutrient deficiencies, endocrine disruptors, chronic inflammation — are entirely absent from the prophylactic mastectomy risk-benefit equation.
Moreover, the rhetoric of BRCA in a cancer-phobic patient generates a cascade of stress physiology that is not benign. Studies show that low perception of control — the defining psychological signature of genetic determinism — is associated with greater cancer recurrence and cancer deaths.[14]

The clinical data behind this is stark: women with false-positive mammography findings — even after being cleared of cancer — showed psychospiritual damage across 12 measurable outcomes equivalent to an actual breast cancer diagnosis, with suicide risk spiking 16-fold and cardiac death risk rising 26.9-fold in the week following a positive result. The full documentation is in our foundational investigation: "'Hidden Dangers' of Mammograms Every Woman Should Know About."
The fear that a BRCA diagnosis provokes triggers “aberrant secretion of stress hormones which further magnifies risk in a vicious cycle” — the diagnosis can become causally implicated in the very disease progression it purports to prevent.[9]
The full radiobiological evidence base is catalogued in the GreenMedInfo X-Ray Mammography Dangers Database.
V. The Profitable Cascade
Why Overdiagnosis Persists When the Evidence Is Clear
The overdiagnosis literature is not obscure. It has been published in the New England Journal of Medicine, The Lancet, the British Medical Journal, and the Cochrane Collaboration — the gold standard of evidence synthesis — has explicitly stated that for every woman who avoids a breast cancer death through mammography, approximately ten are unnecessarily diagnosed and treated.[6] This ratio has been known for years. And yet the screening machinery continues.

In 2018, Goldman Sachs issued an internal report asking whether curing patients was a “sustainable business model,” noting that one-shot cures “quickly exhaust recurrent revenue streams.”[15] The mammography-to-treatment pipeline illustrates the point precisely: screening mammograms generate revenue. Abnormal findings generate diagnostic mammograms. Biopsies generate DCIS diagnoses. DCIS diagnoses generate surgeries. Surgeries generate radiation. Radiation generates follow-up imaging. Hormone suppression therapy generates five to ten years of pharmaceutical revenue. A woman who is overdiagnosed with DCIS and overtreated is not a failure of the system — she is, in a precise financial sense, the system working as designed.[16]

This profit architecture has a origin story: Breast Cancer Awareness Month itself was co-founded in 1985 by Imperial Chemical Industries — a manufacturer of carcinogenic chemicals including paraquat and trichloroethylene — whose pharmaceutical division stood to profit from every mammogram that generated a diagnosis requiring treatment. The same company that may have contributed to the breast cancer epidemic helped design the awareness campaign that never once mentioned the word carcinogen. The full investigation is in “Stop Pinkwashing: The Truth Breast Cancer Charities Bury.”
For the complete evidentiary case — including the COMET trial, the DCIS radiation irony, and the 20-footnote scientific record — see "The Cancer Deception."
VI. The Biology That Goes Unasked
Why Does Breast Tissue Become Cancer-Permissive?
The New Biology — the emerging synthesis of epigenetics, microRNA biology, microbiome science, and systems physiology — offers a framework for the question that mammography screening never asks: why does breast tissue become cancer-permissive in the first place?
The answers are increasingly specific. The Western Pattern Diet generates chronic systemic inflammation through multiple intersecting mechanisms. Gluten-containing grains drive intestinal hyperpermeability, allowing bacterial endotoxins to translocate into systemic circulation and trigger persistent immune activation — providing an oncogenic microenvironment.[1] Conventional dairy products deliver exosomes that skew immune differentiation toward the pro-inflammatory Th17 lineage.[17]
Meanwhile, the microRNAs present in cruciferous vegetables — particularly a broccoli-derived microRNA recently shown to inhibit breast cancer cell growth through its effect on the TCF7 gene[18] — are absent from processed food. The food environment is not a background variable in breast cancer risk. It is an active upstream determinant. Completely unaddressed by any screening guideline, any USPSTF grade, or any political debate about task force membership.
Endocrine-disrupting chemicals — phthalates, bisphenol A, synthetic estrogens from plastics and personal care products — are documented drivers of epigenetic dysregulation in breast tissue, capable of altering gene methylation patterns and activating oncogenic pathways.[19] Exposure to these compounds can reprogram the germline — affecting not just the exposed individual but subsequent generations.[20] This is the biology of breast cancer prevention. None of it involves a mammography machine.
VII. The Real Crisis
Beyond the Task Force Battle
RFK Jr.’s firings at the USPSTF are alarming if we accept the media’s superficial conventional medical political framings: the replacement of independent scientists with ideological allies represents a real threat to the integrity of public health guidance. If true, and the author believes they are not, these concerns deserve the outrage they have received.
The truth is that there is nothing more MAHA than what Secretary Kennedy is doing. The Make America Healthy Again movement claims to be about root causes — about asking why chronic disease exploded, why the healthcare system produces sickness as reliably as it produces revenue, why the bodies of American women have become a profit center for an industry that begins with a carcinogen and ends with a mastectomy. If that vision means anything, it must mean this: that the most important reform in breast cancer policy is not who sits on the task force, but whether the task force is finally empowered to ask why breast cancer arises in the first place.
Overdiagnosis and overtreatment are not rogue outcomes of a broken system — they are the system operating exactly as designed. Reforming them is not a fringe position. It is the most coherent expression of what a health-first movement could actually accomplish.

But the carefully engineered outrage is effective because it has had a blinding effect. It has made it impossible, in the current political atmosphere, to say what the evidence has been saying for two decades: that the mammography-to-treatment pipeline produces substantial harm alongside its benefits; that overdiagnosis and overtreatment are not edge cases but central features of how the system operates; and that the entire framework of cancer “prevention” has been captured by a detect-and-treat model that leaves the actual causes of cancer entirely intact. And that does not account for the growing body of preclinical and clinical evidence that lifestyle, mindset, natural and integrative medicine has a fast-growing body of compelling research indicating that they may constitute safe, effective, affordable and easily accessible approaches to breast cancer prevention and treatment, as meticulously indexed on projects like my own: GreenMedInfo.com. There are 3,200 studies you can peruse and share below.

The USPSTF — however expertly composed, however methodologically rigorous — grades screening procedures. It does not grade dietary intervention. It does not grade reduction of endocrine-disrupting chemical exposure. It does not grade microbiome restoration. It does not ask why a million American women develop breast cancer each year, or what has changed in their food environment, their toxicant burden, their epigenetic terrain, that makes them susceptible.
Until those questions are asked — and funded, and clinically prioritized — the battle over who sits on the task force is a battle over the rearrangement of furniture in a burning house.
Do dive deeper into chronic conditions like cancer through the lens of the New Biology, read:

Read and share this thread on X:
FOOTNOTES & CITATIONS
[1] Fasano, A. (2012). Leaky gut and autoimmune disease. Clinical Reviews in Allergy and Immunology, 42(1), 71–78. Suzuki, T. (2013). Regulation of intestinal epithelial permeability by tight junctions. Cellular and Molecular Life Sciences, 70(4), 631–659.
[2] Ji, S. (2020). Regenerate: Unlocking Your Body’s Radical Resilience through the New Biology. Hay House. Chapter 1. Dolati et al. (2017). Curcumin restores microRNA expression patterns dysregulated in multiple sclerosis. Journal of Cellular Biochemistry.
[3] Bleyer, A., & Welch, H.G. (2012). Effect of three decades of screening mammography on breast-cancer incidence. New England Journal of Medicine, 367(21), 1998–2005.
[4] Welch, H.G., & Black, W.C. (2010). Overdiagnosis in cancer. Journal of the National Cancer Institute, 102(9), 605–613.
[5] Zackrisson, S., et al. (2006). Rate of over-diagnosis of breast cancer 15 years after end of Malmo mammographic screening trial. BMJ, 332(7543), 689–692. Jorgensen, K.J., & Gotzsche, P.C. (2009). Overdiagnosis in publicly organised mammography screening programmes. BMJ, 339, b2587.
[6] Gotzsche, P.C., & Nielsen, M. (2011). Screening for breast cancer with mammography. Cochrane Database of Systematic Reviews. Gotzsche, P.C. (2012). Mammography screening is harmful and should be abandoned. Journal of the Royal Society of Medicine, 105(2), 51–59.
[7] American Cancer Society. (2024). Breast Cancer Facts & Figures. DCIS accounts for approximately 20% of new breast cancer diagnoses.
[8] Narod, S.A., et al. (2015). Breast cancer mortality after a diagnosis of ductal carcinoma in situ. JAMA Oncology, 1(7), 888–896. Esserman, L.J. (2014). Rethinking screening for breast cancer and prostate cancer. JAMA, 302(15), 1685–1692.
[9] Ji, S. (2020). Regenerate. Part One: ‘Genes load the gun, but environment pulls the trigger.’ On BRCA: ‘epigenetic exposures can knock out the cancer-protective function of the BRCA genes.’
[10] Borzekowski, D.L.G., et al. (2014). The Angelina effect. Genetics in Medicine, 16(7), 516–521. Documents increased BRCA testing and prophylactic mastectomy rates following Jolie’s disclosure.
[11] Copson, E.R., et al. (2018). Germline BRCA mutation and outcome in young-onset breast cancer (POSH). The Lancet Oncology, 19(2), 169–180.
[12] BRCA1 polymorphism K1183R associated with increased breast cancer survival. NCBI PubMed ID: 24600974. Ji, S. (2020). Regenerate.
[13] Brenner, D.J., & Hall, E.J. (2007). Computed tomography — an increasing source of radiation exposure. NEJM, 357(22), 2277–2284. On radiation risk in BRCA-positive women who carry impaired DNA repair capacity.
[14] Henderson, B.N., & Donatelle, R.J. (2002). The relationship between cancer locus of control and CAM use. Psycho-Oncology, 12(1), 59–67. Low perceived control associated with greater recurrence and psychiatric morbidity.
[15] Richter, S. (2018). The genome revolution. Goldman Sachs equity research report. Internal analysis cited in Ji, S. (2020). Regenerate, Chapter 1.
[16] Brownlee, S. (2007). Overtreated: Why Too Much Medicine Is Making Us Sicker and Poorer. Bloomsbury. Economic analysis of overtreatment incentive structures.
[17] Exosomal content of commercial dairy and Th17 immune skewing. Ji, S. (2020). Regenerate. NCBI PubMed ID: 25822997.
[18] Broccoli microRNA inhibiting breast cancer via TCF7 gene. Ji, S. (2020). Regenerate, Chapter 2. Endnote fn. 89.
[19] Soto, A.M., & Sonnenschein, C. (2010). Environmental causes of cancer: endocrine disruptors as carcinogens. Nature Reviews Endocrinology, 6(7), 363–370.
[20] Anway, M.D., et al. (2005). Epigenetic transgenerational actions of endocrine disruptors and male fertility. Science, 308(5727), 1466–1469.
Adapted from Regenerate: Unlocking Your Body’s Radical Resilience through the New Biology by Sayer Ji (Hay House, 2020). GreenMedInfo.com.
No hay comentarios:
Publicar un comentario