Jun 19, 2026

A drug sold as harmless turns out to wound the gut, the heart, the kidney, and the very ecology within us. Here is the full ledger — and the plants that heal without a bill coming due.
“A foreign compound the body has no use for — and no fluent grammar to read — is not neutral. It is a stranger handed the keys to every room in the house.” ~ REGENERATE
There is a word that pharmacology uses with great precision and almost no public attention: xenobiotic. From the Greek xenos, stranger, and bios, life. A xenobiotic is a chemical foreign to the living system — a molecule that nothing in three billion years of evolution prepared the body to metabolize, recognize, or befriend. Ibuprofen is a xenobiotic. So is acetaminophen. So is the entire class of synthetic painkillers that a quarter of the adult population reaches for on any given week, as casually as one reaches for water.
We have been taught to think of these drugs as the safe ones. The over-the-counter ones. The ones you can hand to a teenager with a headache, keep in the glovebox, take “as needed” for years without a second thought. This is the most successful piece of misdirection in modern pharmacology — and the literature, if you actually read it, tells a far darker and more interesting story.
I want to lay out that story plainly. Not to frighten you, but because I think the truth here is genuinely clarifying: it reveals the deep logic of why synthetic medicine so often wounds while plant medicine so often blesses. The difference is not sentimental. It is structural. It is written into the chemistry itself.
I. The Ledger Nobody Reads: What Ibuprofen Actually Does
Let me begin where the drug companies would prefer we never linger — with the documented harms. Not folklore, not anecdote. Peer-reviewed, FDA-acknowledged, repeatedly replicated harm.
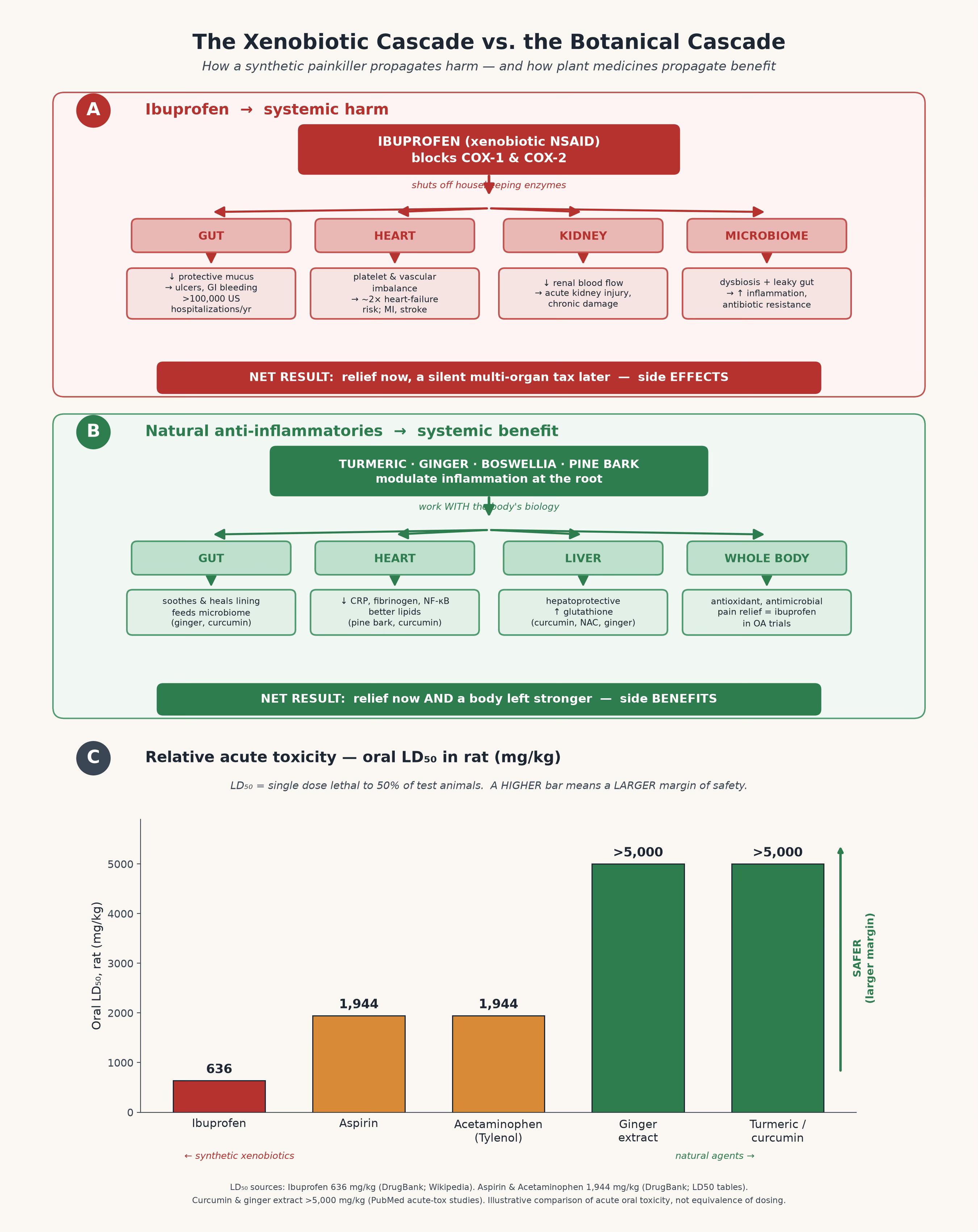
Ibuprofen works by blocking the COX enzymes (cyclooxygenase-1 and -2). This is presented as elegant: shut down the inflammatory cascade, and pain quiets. But COX-1 is not a “pain enzyme.” It is a housekeeping enzyme — it maintains the protective mucus lining of your stomach, regulates blood flow to your kidneys, and governs the platelet behavior that keeps your cardiovascular system in balance. To block it for pain is to switch off a dozen quiet, vital functions in order to silence one loud one. This is the xenobiotic’s signature move: it cannot be specific, because the body never built a specific lock for this foreign key (GreenMedInfo, “Newly-Identified Side Effects of Ibuprofen and 20 More Reasons to Be Cautious”).
Here is the ledger, drawn from the published record:
The gut bleeds. NSAID use causes gastrointestinal ulceration, bleeding, and perforation — accounting for more than 100,000 hospitalizations in the United States every year (Bhala et al., The Lancet, 2013;382(9894):769–79).
The heart suffers. Ibuprofen raises the risk of heart attack, stroke, sudden cardiac arrest, and roughly doubles the risk of heart failure in regular users (BMJ, 2016 — analysis of ~10 million users). A large European study tied current NSAID use to a 19% higher risk of hospitalization for heart failure (TCTMD coverage of the BMJ analysis).
The kidneys fail. Because ibuprofen constricts the vessels feeding the kidney, it can precipitate acute kidney injury and chronic renal damage — especially in the dehydrated, the elderly, and the athletic.
Pregnancy is endangered. First-trimester use is associated with a doubling of miscarriage risk.
And the rare-but-catastrophic: drug-induced hepatitis, toxic epidermal necrolysis, aseptic meningitis, esophageal perforation, hypertension, asthma exacerbation, hearing loss, and reduced male fertility (GreenMedInfo “20 More Reasons”).
That last list is not theoretical. Aseptic meningitis was the newly identified entry that prompted the most recent review — documented in a 2024 case report in Cureus (Kalfoutzou et al., Cureus, 2024; DOI:10.7759/cureus.65936).
Now sit with the toll in aggregate. NSAIDs as a class are responsible for an estimated over one million hospitalizations and up to 165,000 deaths every year worldwide (Conaghan, Rheumatology International, 2012). This is not the body count of a fringe drug. This is the body count of the medicine in your kitchen drawer.
II. The Underreporting Machine
Here is the part that should genuinely unsettle you — not the harms themselves, but how invisible they are made to be.
The FDA’s adverse-event reporting system (FAERS) is the official ledger of drug harm in America. And by the agency’s own acknowledgment, it captures only a small fraction — on the order of 1 to 10 percent — of the adverse events that actually occur. Reporting is voluntary. A bleeding ulcer in a 70-year-old who took ibuprofen for arthritis is almost never traced back to the drug and logged. A heart-failure hospitalization is filed under “heart failure,” not “iatrogenic NSAID injury.” The death certificate says “GI hemorrhage,” not “Advil” (GreenMedInfo “20 More Reasons”).
So the numbers you just read — the million hospitalizations, the 165,000 deaths — are not the ceiling. They are the visible tip. The structure of the surveillance system guarantees that the true harm is systematically undercounted, while the benefit is amplified through billions of dollars in advertising. Underreported in their downsides, over-promoted in their upsides — that asymmetry is not an accident of the system. It is the system.
We need only remember Vioxx — a sister NSAID withdrawn in 2004 after it was estimated to have caused somewhere between 88,000 and 140,000 cases of serious heart disease before regulators acted (GreenMedInfo, “A Powerful Aspirin Alternative Grows on Trees”). The data existed for years. The drug stayed on the shelf. The class did not learn the lesson; it simply rotated the molecule.
III. The Class, Not the Compound: Why the Whole Family Is Toxic
Here is the thesis I most want you to carry away, because it is bigger than ibuprofen.
The problem is not that we picked the wrong synthetic painkiller. The problem is the category. These drugs are xenobiotics — strangers to the body — and a stranger, however useful in one narrow function, cannot help but disturb the rooms it was never invited into. The toxicity is not a bug to be engineered out in the next molecule. It is the inheritance of foreignness itself.
Consider the two giants of the over-the-counter aisle, and notice that each poisons a different organ while wearing the same friendly mask:
Ibuprofen (and the NSAIDs) damage the gut, heart, and kidney — by blocking the housekeeping enzymes that protect them.
Acetaminophen (Tylenol/paracetamol) is the leading cause of acute liver failure in the Western world — and, as I have documented at length, it does something stranger still: it blunts the human capacity for empathy. A single standard dose measurably dampens a person’s emotional response to the suffering of others, dulls positive feeling, and increases risk-taking — by quieting the same brain regions (the anterior insula and anterior cingulate cortex) that let us feel with one another (Sayer Ji, “Tylenol: From Painkiller to Empathy Killer”).
Read those two together and the pattern resolves. One drug ulcerates the gut and strains the heart. The other dissolves the liver and erodes compassion itself. These are not isolated quirks of two unlucky molecules. They are two faces of a single fact: when you introduce a foreign compound the body cannot read, it will exact a price somewhere — and that price will be paid in a currency the drug’s marketing never names. I have written about the broader sweep of this in The Mind Thieves: How 6 Common Medications Are Stealing Our Humanity— because once you see it in painkillers, you begin to see it everywhere.
And the price keeps revealing new dimensions. Recent work shows that long-term ibuprofen use alters cardiac signaling at recommended doses — disturbing aerobic respiration and raising oxidative stress in the heart muscle itself (American Physiological Society, 2024). And in perhaps the most haunting finding of the past two years: common painkillers including ibuprofen and acetaminophen have been shown to supercharge antibiotic resistance — driving bacteria to mutate faster and become harder to kill (ScienceDaily, August 2025; npj Antimicrobials and Resistance, 2024). The stranger in the house, it turns out, has been teaching the other strangers how to fight back.
IV. The Ecology Within: How Ibuprofen Wounds the Microbiome
There is one harm that deserves its own section, because it reframes everything.
We now know that ibuprofen does not merely irritate the stomach lining mechanically. It disrupts the gut microbiome — the trillions-strong ecology of organisms that constitute most of the cells we carry and a great deal of who we are. NSAIDs shift the microbial balance, increase intestinal permeability (the condition popularly called “leaky gut”), and promote the overgrowth of inflammatory species such as Enterobacteriaceae (Frontiers in Pharmacology, 2020; Frontiers in Cellular and Infection Microbiology, 2021).
Consider the cruel circularity of this. You take ibuprofen for inflammation. The drug degrades the gut barrier and tips the microbiome toward inflammatory species. The leaking barrier and the disturbed ecology generate more systemic inflammation. You reach for another dose. The xenobiotic does not resolve the fire — it quietly feeds the conditions that keep it burning, while numbing your awareness of the smoke.
This is the antithesis of how a plant medicine behaves. A plant, having co-evolved within the same web of life as your microbiome, tends to feed that ecology rather than scorch it. Which brings us, at last, to the other side of the scale.
The anatomy of an alternative. Curcuma longa dissected in the manner of a 19th-century botanical plate — rhizome, root, and the curcuminoid pigments that quiet inflammation as effectively as ibuprofen in head-to-head trials, while protecting the very organs the drug endangers.
V. For Those Who Cannot Yet Let Go: Reducing the Toll

Before the alternatives, a word of mercy — because I know many readers are dependent on these drugs, or care for someone who is, and cannot simply stop tomorrow, because they do actually effectively ‘kill pain.’ The literature offers something genuinely useful here: a body of evidence on natural agents that blunt the toxicity of NSAIDs and acetaminophen while you reduce reliance. This is harm reduction, grounded in the science of NSAID-induced toxicity mitigation.
To protect the gut against NSAID injury, the evidence points to:
Probiotics (Lactobacillus species), which restore the microbial balance the drug disrupts.
Phosphatidylcholine, which reinforces the very mucus barrier ibuprofen strips away.
Vitamin C, sulforaphane (from broccoli sprouts), astaxanthin, honey, apple polyphenols, cardamom, basil, and fucoidan — each shown to reduce gastric damage from aspirin/NSAIDs.
To protect the liver against acetaminophen injury, the literature is even richer:
N-acetylcysteine (NAC) — already the hospital antidote for Tylenol overdose, and the precursor your body uses to make glutathione, the master detoxifier.
Silymarin (milk thistle), curcumin, 6-gingerol (ginger), alpha-lipoic acid, CoQ10, berberine, black seed (Nigella sativa), and grape seed extract — all documented to defend the liver against paracetamol toxicity.
Notice what is happening here. The plants do not merely counteract a poison. They restore the gut barrier, rebuild the antioxidant reserves, feed the microbiome, support the liver’s own machinery. Even in the role of damage control, the natural agent works by strengthening the body — never by adding a second stranger to fight the first.
VI. The Garden’s Answer: Relief With Side Benefits, Not Side Effects
And now the heart of it. If the synthetic painkiller is a stranger that silences pain by disabling the body, the plant is a relative that resolves pain by informing the body. The alternatives are not weak consolation prizes. In head-to-head trials, several are the equal of the drug — without the ledger of harm.
Turmeric / curcumin. In a randomized controlled trial of knee osteoarthritis, curcumin extract was found as effective as ibuprofen for pain relief — with significantly fewer gastrointestinal side effects (Kuptniratsaikul et al., Clinical Interventions in Aging, 2014; ClinicalTrials.gov NCT00792818). The plant that matches the drug for arthritis also protects the liver, feeds the microbiome, and quiets systemic inflammation at the root.
Ginger. A potent anti-inflammatory and analgesic with millennia of use, ginger inhibits the same inflammatory pathways as NSAIDs — while soothing the gut rather than ulcerating it (GreenMedInfo “20 More Reasons”).
Boswellia serrata (frankincense). It inhibits the 5-LOX inflammatory pathway — a route NSAIDs miss entirely — and is well-documented for arthritis and inflammatory pain.
Pycnogenol (French maritime pine bark). A genuine aspirin alternative: it inhibits both COX-1 and COX-2 within thirty minutes, lowers C-reactive protein, NF-κB, fibrinogen, and matrix metalloproteinases — and in clinical study proved superior to aspirin at preventing smoking-induced clotting, with no increase in bleeding time (GreenMedInfo, “A Powerful Aspirin Alternative Grows on Trees”; Thrombosis Research, 1999). Aspirin thins the blood and erodes the stomach. The pine bark calms the same clotting cascade — and leaves the gut intact.
This is the phrase I keep returning to, and I will say it plainly: the natural medicines come with side benefits, not side effects. Take ibuprofen and the gut, heart, and kidney are collateral damage. Take turmeric and the “collateral” is an improved lipid profile, a calmer microbiome, a protected liver, a brain bathed in an anti-inflammatory compound. The drug subtracts. The plant adds. One leaves you with a debt; the other leaves you with a dividend.
VII. The Deeper Reading
Step back, and the contrast resolves into something almost philosophical.
A xenobiotic painkiller is the chemical embodiment of a worldview — the belief that the body is a machine with faulty parts, that pain is a signal to be suppressed rather than understood, and that healing is something imposed from outside by a force foreign to life. It silences the smoke alarm and calls the room safe. And because it is a stranger, it cannot do its one job without disturbing every other room it passes through.
The plant carries the opposite worldview in its very chemistry. Having grown within the same living web as the body it heals — sharing membranes, enzymes, evolutionary grammar — it does not silence the alarm but addresses the fire. It is legible to us in a way the synthetic molecule can never be. That legibility is precisely why its “side effects” so often turn out to be benefits: the body recognizes the plant as kin, and metabolizes the encounter into health rather than harm.
We were sold a bargain we did not understand. We traded a moment’s relief for a slow, silent, underreported tax on the gut, the heart, the kidney, the liver, the microbiome — and, with the empathy-dimming cousins, on the very faculties that make us human. It was never a good trade. And the most quietly radical thing you can do is to notice that the better answer was growing in the garden the entire time — offering its relief freely, with a dividend instead of a debt.
The willow knew. The turmeric root knew. The pine bark knew. We are, at best, still learning to read what they have been saying all along.
A note on practice
This essay is a meditation on what the science reveals, not medical advice. Do not stop a prescribed medication abruptly, and never discontinue any drug — including over-the-counter painkillers used for a diagnosed condition — without a knowledgeable practitioner’s guidance. Some of the natural agents named here interact with medications (curcumin, ginger, and pycnogenol can affect blood clotting; high-dose botanicals can affect the liver and kidneys). Pregnancy, kidney disease, bleeding disorders, and polypharmacy all demand professional oversight. Honor the power of these plants by respecting it.
Sources & further reading
The harms of ibuprofen and the NSAID class
Newly-identified side effects and the full harm ledger — Sayer Ji, GreenMedInfo: “Newly-Identified Side Effects of Ibuprofen and 20 More Reasons to Be Cautious”
GreenMedInfo research database — Ibuprofen toxicity (19 studies)
GI bleeding, vascular and cardiac risk meta-analysis — Bhala N, et al. “Vascular and upper gastrointestinal effects of NSAIDs.” The Lancet, 2013;382(9894):769–79.
Global NSAID mortality and morbidity — Conaghan PG. “A turbulent decade for NSAIDs.” Rheumatology International, 2012;32:1491–1502.
Aseptic meningitis case report — Kalfoutzou A, et al. Cureus, 2024. DOI: 10.7759/cureus.65936
Heart failure risk (~10 million users) — BMJ, 2016;354:i4857; TCTMD coverage
Long-term cardiac signaling damage at recommended doses — American Physiological Society, 2024
The gut and the microbiome
NSAIDs and the gut microbiota — Frontiers in Pharmacology, 2020;11:1153
Ibuprofen, intestinal permeability, and Enterobacteriaceae — Frontiers in Cellular and Infection Microbiology, 2021
Antibiotic resistance (2024–2025)
“Painkillers supercharge superbugs” — ScienceDaily, August 2025
Underlying study — npj Antimicrobials and Resistance, 2024
The xenobiotic-class argument (acetaminophen / Tylenol)
Sayer Ji, Substack: “Tylenol: From Painkiller to Empathy Killer”
Sayer Ji, Substack: “The Mind Thieves: How 6 Common Medications Are Stealing Our Humanity”
Acetaminophen blunts empathy — Mischkowski D, Crocker J, Way BM. “From painkiller to empathy killer.”Social Cognitive and Affective Neuroscience, 2016. DOI: 10.1093/scan/nsw057
Acetaminophen reduces positive empathy — Frontiers in Psychology, 2019
Reducing toxicity for the dependent
GreenMedInfo research database — NSAID-induced toxicity: protective natural agents (46 studies)
Natural alternatives
Curcumin as effective as ibuprofen for knee osteoarthritis — Kuptniratsaikul V, et al. Clinical Interventions in Aging, 2014;9:451–8. Trial: ClinicalTrials.gov NCT00792818.
Pycnogenol as an aspirin alternative — Sayer Ji, GreenMedInfo: “A Powerful Aspirin Alternative That Grows on Trees”
Pycnogenol vs. aspirin for smoking-induced clotting — Thrombosis Research, 1999;95(4):155–61
GreenMedInfo popular research index — Most popular natural-health research
No hay comentarios:
Publicar un comentario